Our patient is a 29 year-old female, a professional fencer since the age of 11, who came to us with right-sided hip pain. She denied any past trauma, and at the time of her visit she had just recovered from COVID. She had been diagnosed with femoroacetabular impingement (FAI), and had undergone 4 months of physical therapy, with no improvement. Doctors had recommended arthroscopic surgery but she declined based on supporting scientific evidence and the opinions of other clinicians.
The Challenge
The patient’s pain had devolved from her initial symptoms, and she now reported swelling and tenderness in her hip region, and restrictive pulling sensations with every step. A surgeon referred her for MRI, but the results did not reveal anything new. He administered steroid injections, which didn’t help.
Our Diagnostic Process
Clinical Examination
Our physical exam revealed a small nodule that when palpated reproduced her pain gave a positive tinel’s sign – a referred pins-and-needles sensation elicited by tapping on the nerve. Our clinical tests confirmed a classic presentation of FAI.
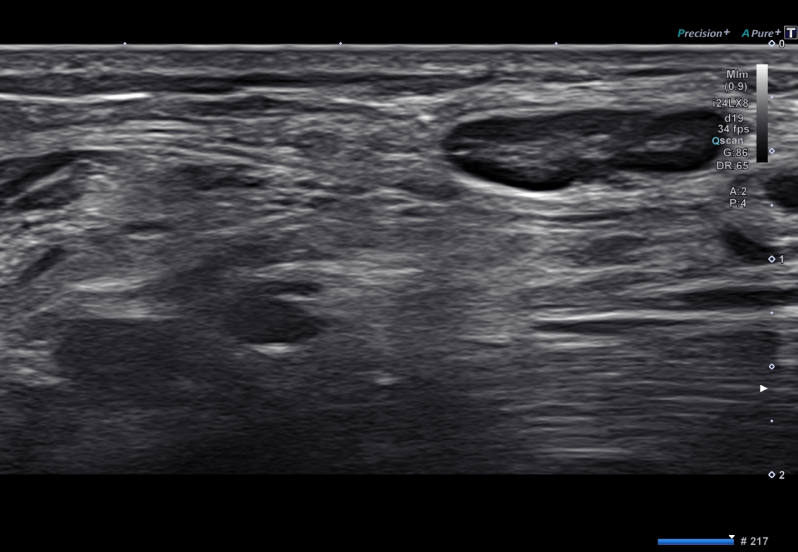
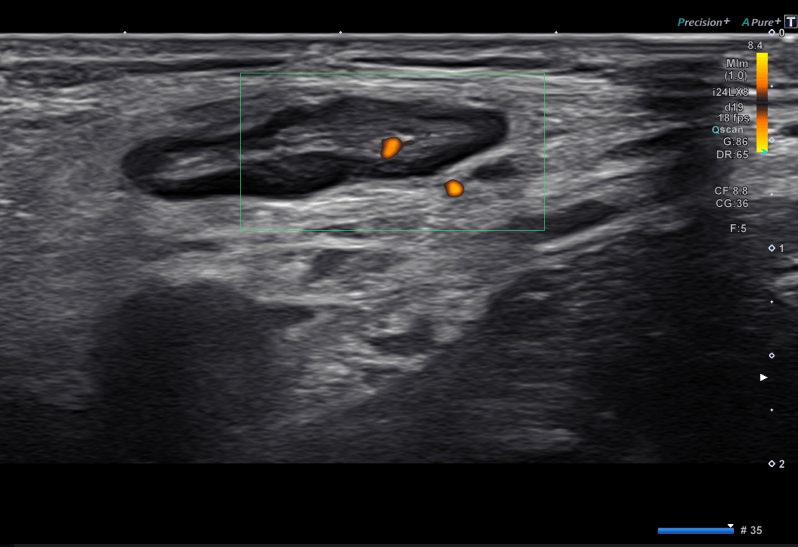
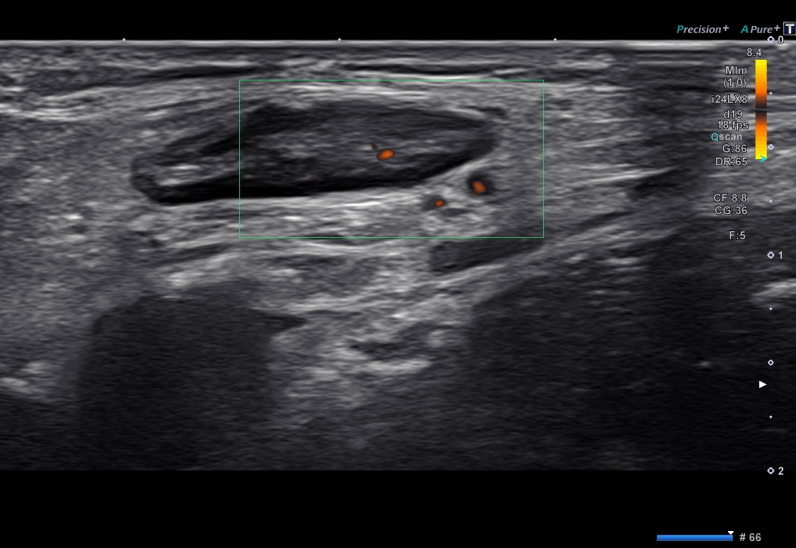
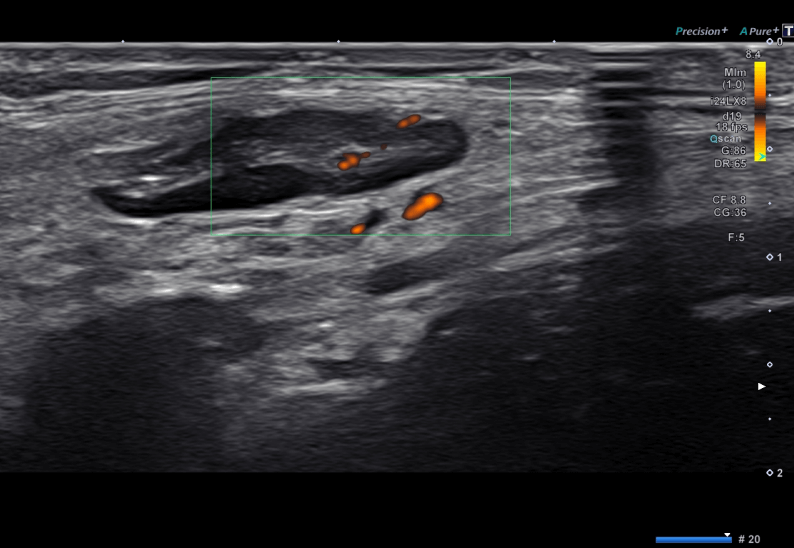
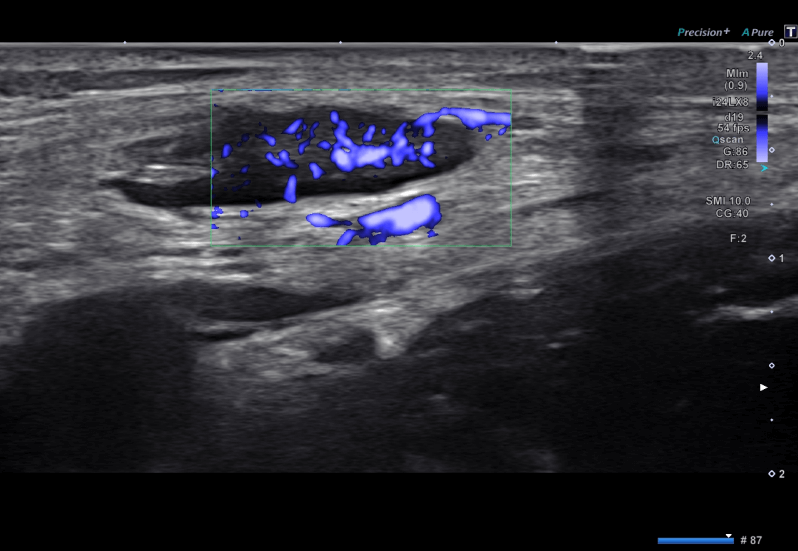
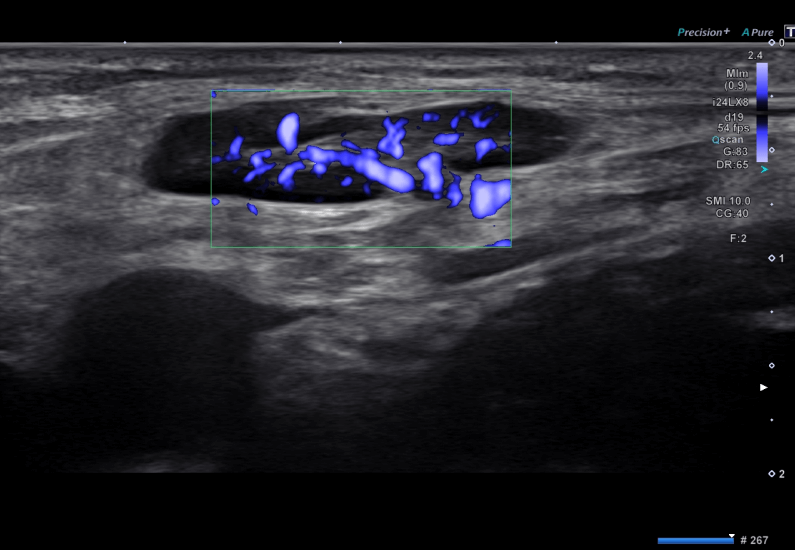
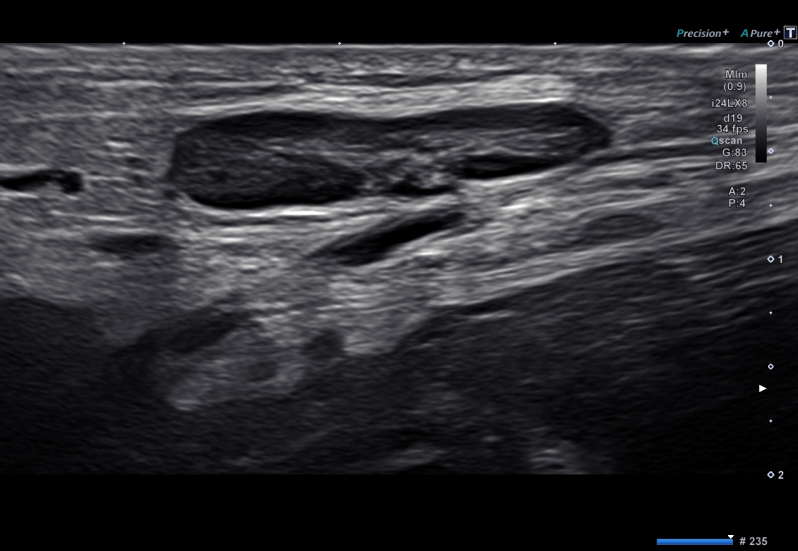
High Resolutions Ultrasonography Diagnostic Exam
Our initial findings concurred with the patient’s two previous MRIs, but we also found severe tendinopathy of the reflected head of rectus femoris, which is typically missed on MRI. We also found a large swollen lymph node at the locus of discomfort, with positive microvascular flow indicating inflammation. The lymph node was so enlarged that it was pressing on the femoral nerve. The node appeared to be benign, but we decided to do some precautionary blood work, which came back negative. Her primary care physician suggested that the swollen node was due to her recent COVID infection.
Discussion
When conducting patient exams, it is important for doctors to consider the patient’s overall health. High resolution ultrasonography is superior to MRI for examining soft tissues and nerves, and for dynamic imaging of the structures in motion. Its capabilities for Power Doppler, superb microvascular imaging (SMI), and sonoelastography are also clinically beneficial. In the hands of an experienced clinician, diagnostic ultrasound provides a more precise examination based on the patient’s unique profile.
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating the full thickness tear and already occurring muscle atrophy due to misdiagnosis and not referring the patient to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed to be a complete tear with muscle contraction under diagnostic sonography (not possible with MRI)
Complete tear of rectus femoris with large hematoma (blood)
Separation of muscle ends due to tear elicited on dynamic sonography examination