
Calcific Tendinopathy Treatment
Personalized boutique services supported by cutting-edge
integrative diagnostics and advanced holistic therapies.
Dr. Kalika and Dr. Brosgol Team Up for Next-
Level Tendinopathy Treatment

Clinical director & DC RMSK
Verified Expert Profiles
Dr. Lev Kalika, DC, RMSK, founder and clinical director of NYDNRehab, has 25 years of hands-on clinical experience, helping patients to overcome physical pain syndromes and movement disorders. His expertise in rehabilitative medicine has helped countless athletes to heal and rehabilitate sports injuries, and return to play at pre-injury performance levels.
Dr. Kalika is an expert in diagnostic musculoskeletal ultrasonography, giving NYDNRehab a distinct advantage in on-site diagnostics and progress monitoring. In addition to his clinical practice, Dr. Kalika frequently conducts and publishes peer-reviewed research on ultrasound-guided procedures. Dr. Kalika’s expertise in tendinopathy treatment is second to none in NYC.

Dr. Yuri Brosgol, MD is a neurologist with 25+ years of experience in treating myofascial and chronic pain conditions. Thanks to guidance by high resolution ultrasound that provides advanced anatomical and fascial details, Dr. Brosgol’s approach to orthobiologic procedures ensures precision injections for optimal results.
Dr. Brosgol’s expertise provides a holistic and nuanced approach to common sports injuries and orthopedic issues. His expertise in neurology and functional medicine is especially geared to treating chronic pain syndromes.
Together, Dr. Kalika and Dr. Brosgol are revolutionizing the way tendinopathies are diagnosed and treated. The clinic at NYDNRehab features some of the most advanced technologies and therapies currently available for musculoskeletal rehabilitation.
Calcific Tendinopathy: What is it and
how does it develop?
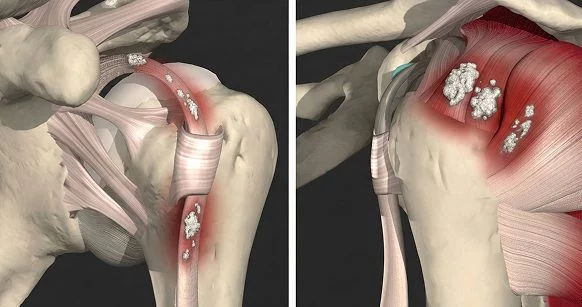
Calcific tendinopathy (also called calcific tendinitis) is a condition where calcium deposits (hydroxyapatite crystals) build up inside a tendon, causing pain and inflammation, and often limiting movement. Despite the condition being fairly common, its origins are poorly understood.
Calcification occurs most often in the rotator cuff tendons of the shoulder, especially the supraspinatus, but it can affect tendons anywhere in the body. A 2024 systematic review highlighted the prevalence of atypical (non-rotator cuff) cases occurring in the spine (~27%), the foot/ankle (~24%), and the hip (~22%).
- Adults aged 30-50
- More common in women, with a female to male ratio of about 80:20
- Patients with metabolic disorders like diabetes are at higher risk
- Frequently develops in patients with low thyroid or other endocrine disorders
Calcific tendinopathy progresses slowly over the course of several months or even years, and typically
presents in 4 distinct stages:
Formative stage
where calcium crystals are deposited, gradually growing in size. Deposits have a chalk-like consistency and are well defined. Pain at this stage is mild, or sometimes non-existent.
Resting stage
where the calcium deposits stop growing and the condition stabilizes.
Resorptive stage
the most acute and painful stage, where the body begins to reabsorb the calcium deposits. As deposits break down, they transform to a toothpaste-like consistency. This stage is marked by intense pressure in the affected tissue, along with intense pain, and it often involves secondary bursitis.
While about 80 percent of calcific tendinopathy cases occur in the shoulder, it can also develop in other joints, including the spine, elbow, hip, knee, ankle and foot. Less common sites are frequently misdiagnosed, leading to mistreatment and unsatisfactory patient outcomes.

Calcific Tendinopathy Symptoms
- Intense pain or burning sensation
- Pain that intensifies during physical activity
- Pain at night that disrupts sleep
- Stiffness and reduced range of motion
- Tenderness to touch in the affected tissues
- Loss of strength
Calcific Tendinopathy and Sports Performance
Calcific tendinopathy can significantly impact sports performance, primarily due to severe pain, reduced range of motion, weakness, and reduced tendon function. The condition can be severely disabling, especially during the acute resorptive phase, forcing athletes to reduce training, modify activities, or take time away from active play.
Calcific tendinopathy is especially disruptive for athletes in overhead or high-impact sports due to repetitive stress that exacerbates symptoms. Sites most commonly affected include the rotator cuff, gluteus medius, quadriceps, and Achilles tendon.
Site-specific impact on sports performance:
| Site | Common Sports Affected | Performance Effects | Typical Severity/ Recovery Notes |
|---|---|---|---|
| Shoulder (Rotator Cuff, esp. supraspinatus) | Throwing (baseball, softball), overhead (tennis, volleyball, swimming), weightlifting | Overhead motion pain/weakness → reduced throwing velocity, serve power, stroke strength; impingement-like symptoms during reps or competition. | Most studied; acute phases highly disabling for upper-body sports. |
| Hip (Gluteus medius/minimus) | Running, soccer, basketball, hockey (lateral movements) | Lateral hip pain, abductor weakness → altered gait, reduced sprint speed, poor lateral stability/cutting; limping or antalgic gait. | Can mimic greater trochanteric pain; impacts agility/endurance sports. |
| Knee (Patellar/Quadriceps tendon) | Jumping (volleyball, basketball), running/sprinting | Anterior knee pain with loading → decreased jump height, slower acceleration, reduced explosive power; high-impact intolerance. | Common in “jumper’s knee” variants; affects plyometrics heavily. |
| Achilles | Running (distance/track), jumping, court sports (tennis, soccer) | Heel/insertional pain → shortened stride, reduced push-off power, slower speeds; high-impact activities exacerbate (e.g., acceleration, hills). | Prevalent in runners/military athletes; can cause functional tendon shortening. |
Diagnosing Calcific Tendinopathy
Effective treatment requires accurate and thorough diagnosis, and other conditions with similar symptoms must be ruled out. In the shoulder, differentiation must be made between calcific tendinitis and dystrophic calcifications – calcium deposits in degenerative or necrotic tissue. Subacromial bursitis and supraspinatus rupture must also be ruled out.
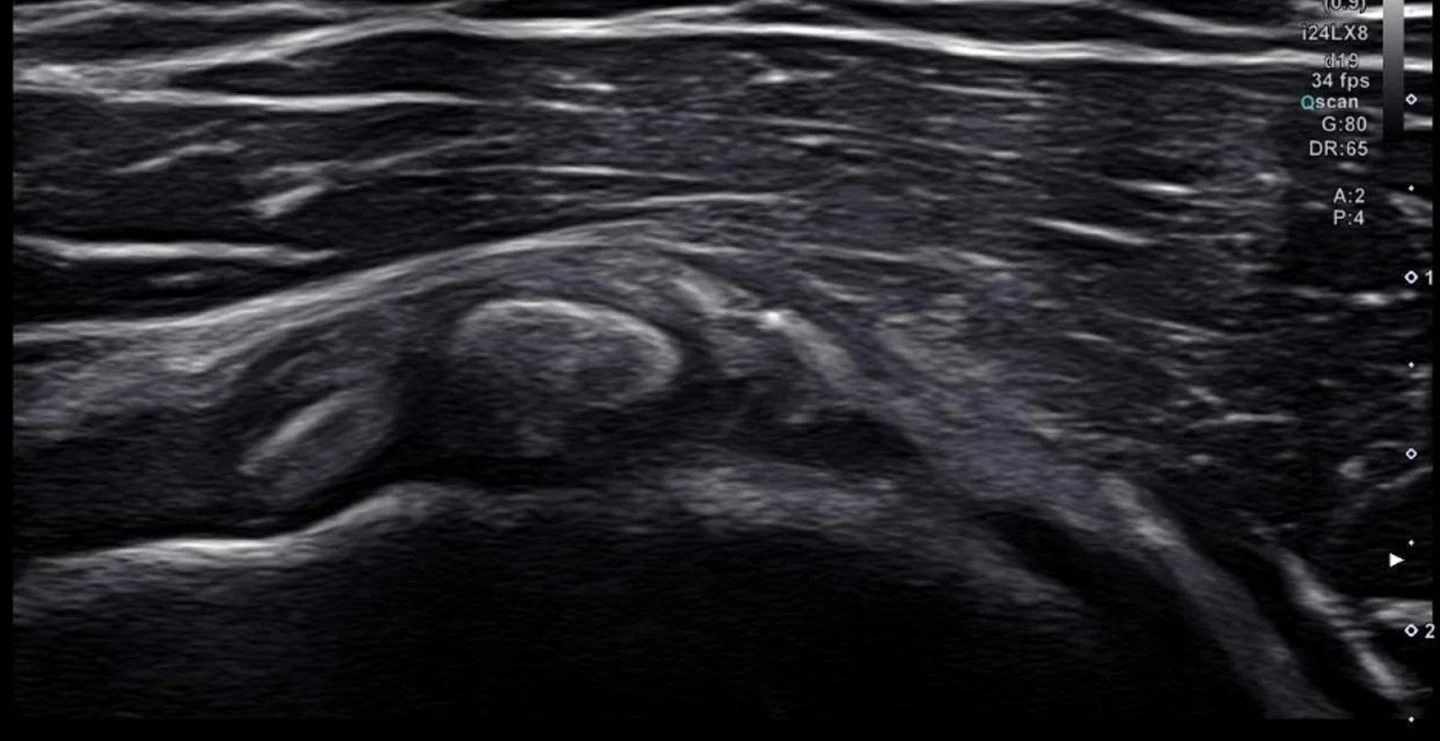
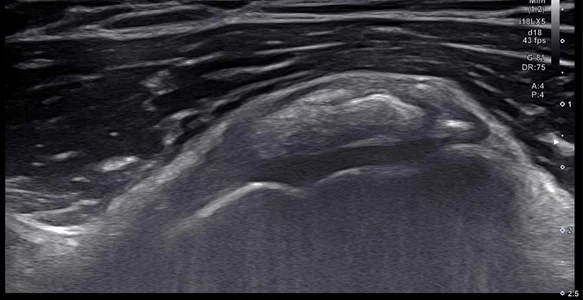
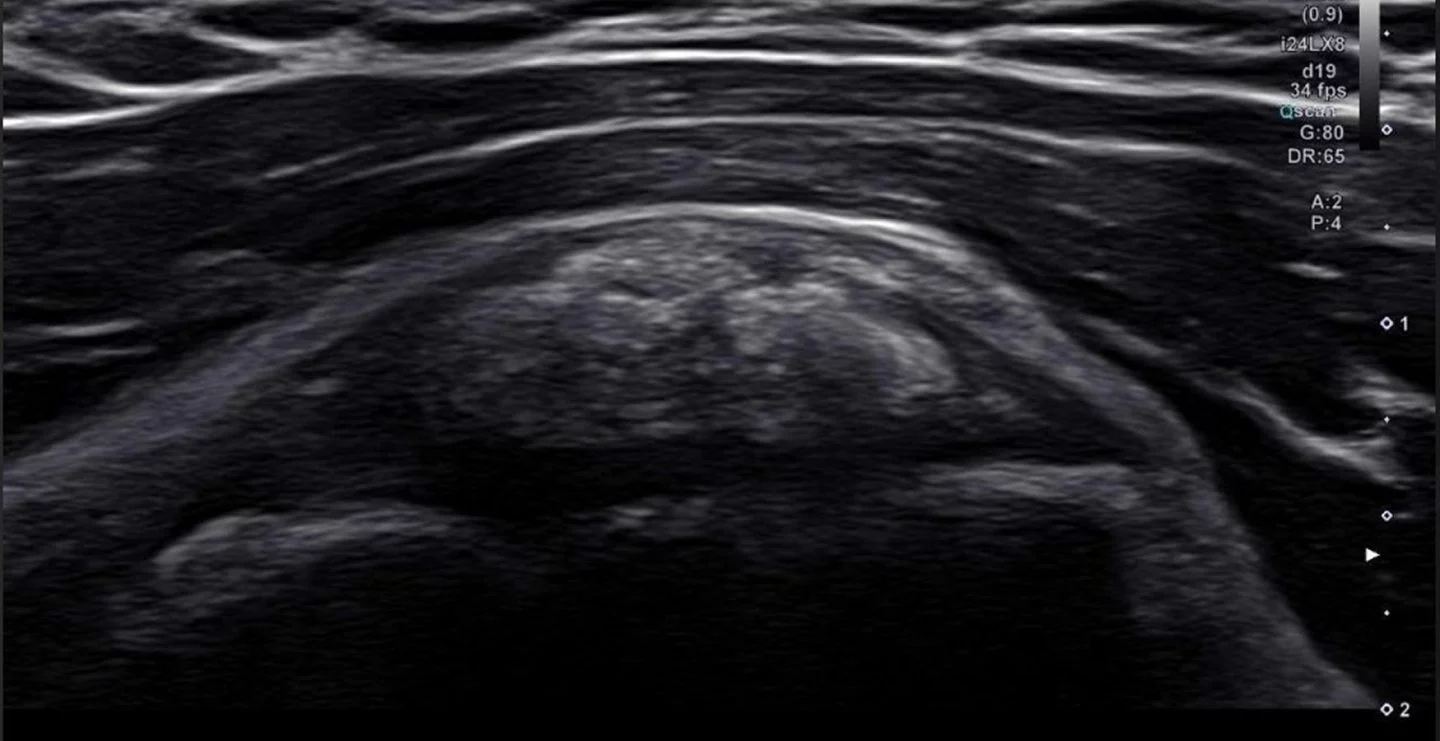
For diagnosis, a combination of x-ray and diagnostic ultrasound is ideal. X-rays allow us to visualize and classify calcium deposits, while ultrasound helps us to dynamically explore the affected tissues, to identify secondary issues such as bursitis and impingement brought on by calcification. Ultrasound also helps us to monitor progress in response to treatment, and assists in guiding treatment procedures.
The clinic at NYDNRehab features the highest resolution ultrasonography currently available. Not only does it allow us to visualize calcium deposits, but it gives us the capability to measure tissue stiffness via sonoelastography, and to visualize microvascular blood flow during various stages of the disease via superb microvascular imaging (SMI).
Advanced Calcific Tendinopathy Treatment at
NYDNRehab
Treatment of calcific tendinopathy varies, depending on the stage of tissue calcification. Conventional treatment emphasizes conservative care in the early stages, often involving NSAIDs and anti-inflammatory medications to relieve pain and inflammation, along with therapeutic ultrasound, microwave diathermy, and iontophoresis – a procedure that uses mild electrical current to push ionized substances through the skin. But conventional approaches only work in less than five percent of cases.
In the early stages of calcific tendinopathy, calcium deposits are soft, making them easier to treat. By starting treatment with pain management, an opportunity is missed to eradicate calcium deposits before they harden.
At NYDNRehab, we begin treatment as soon as we diagnose your condition, using advanced, evidence-based therapies that quickly and effectively eliminate tendon calcium deposits. Two primary approaches have been recognized to provide fast, safe, and effective relief.

ESWT is a non-invasive treatment that delivers high frequency acoustic pulses without breaking the skin tissue barrier. Shockwaves travel through the body’s tissues, creating a therapeutic effect at the interface of musculotendin-bone junction. Shockwaves revascularize damaged tissues to induce healing, and decrease pain signals from hypersensitized nerve endings.
In the case of calcific tendinopathy, shockwaves help to soften calcifications, to be later absorbed, disrupting the connection between small nerves and calcified crystals. Focused ESWT is preferred over radial shockwaves due to their superior quality and anatomical precision. The effectiveness of both high-energy and low-energy focused shockwaves is supported by multiple controlled studies.

Barbotage, also known as lavage, is a minimally invasive procedure used to treat calcific tendinopathy. Barbotage is an outpatient procedure performed under ultrasound guidance in the comfort of our clinic. During the procedure, we locate a calcium deposit in the tendon, then insert a thin needle. The needle is moved back-and-forth, to break up the calcium, and a saline solution is injected to flush it out. Some of the fragments may be aspirated with a syringe. The entire procedure takes between 20-45 minutes.
In some cases, after the calcium deposit has been flushed out, platelet-rich plasma (PRP) is injected into the tendon to promote healing, reduce post-procedure inflammation, and support tendon tissue remodeling.
Preventing Calcific Tendinopathy
Calcific tendinopathy has been associated with metabolic disorders like diabetes, hypothyroidism, and repetitive overuse. Although the exact mechanisms of calcific tendinopathy are poorly understood, there are certain actions you can take to prevent it from developing and progressing.
Actions to avoid calcific tendinopathy:
- Avoid repetitive overuse. Many sports, exercise regimens, and occupations call for repetitive movements under load, but when they start to cause pain, you may be setting yourself up for injury. Never play or work through pain, or mask it with drugs.
- Do regular balanced exercises with good posture and technique, and focus on strengthening muscles that stabilize the joints
- Lose excess body weight to avoid joint overload and metabolic disease associated with obesity.
- Adopt an anti-inflammatory diet rich in leafy greens, vitamin C sources like citrus and broccoli, and pasture-raised animal proteins.
- Stay well-hydrated to support tendon tissues and maintain elasticity.
- Get adequate quality sleep and manage stress.

Range of Available Unique Calcific Tendinopathy
Treatment at Nydnrehab
Calcific Tendinopathy FAQs
While the exact cause is unclear, calcific tendinopathy is thought to involve changes to the tendon, such as degeneration, reduced blood supply, repetitive microtrauma, or metabolic factors. Risk factors include age between 30–60 years, female sex, diabetes, thyroid issues, and sedentary lifestyle.
Calcific tendinopathy is most common in adults aged 30–60, and up to 70% more common in women. It is a fairly common cause of shoulder pain, accounting for up to 40% of all cases. Up to 20% of cases are asymptomatic, so you may have it but not be aware of it.
Calcium deposits can irritate surrounding tissues, cause chemical inflammation, increase pressure within the tendon, or lead to impingement, where soft tissues rub against bone. The resorptive phase triggers intense inflammation as the body breaks down the crystals, generating pain in tender tissues.
Over time, the body often resorbs the calcium deposits naturally, but it can take months or even years. Meanwhile, you are forced to live with pain and reduced mobility. If you have persistent joint pain in your shoulder or elsewhere, it is best to seek professional help early-on.
With conventional medical treatment, your recovery time can take months or even years. But when your calcific tendinopathy is treated with focal shockwave and barbotage, recovery time is much shorter, providing significant relief in a matter of weeks, with full recovery taking from 1-6 months. It is important to follow up with physical therapy to restore optimal function of the affected tissues.





















