Our patient is a 27 year-old male soccer player complaining of persistent low back pain, with difficulty maintaining engagement of the core muscles during high-intensity drills. The patient could not recall an acute injury, but he mentioned a sudden twisting maneuver during a game six weeks prior that “felt off,” although it caused no immediate pain.
Over the following weeks, the athlete noticed that activating his core was becoming progressively more difficult, especially during spriting and rotational actions. He also reported soreness in the lumbar spine and contralateral hip that worsened after training sessions, and posterior chain discomfort during running and cutting maneuvers.
During the clinical exam, we noted poor co-contraction between the anterior abdominal wall and the paraspinal muscles. We also discovered altered breathing mechanics, with reduced lateral expansion.
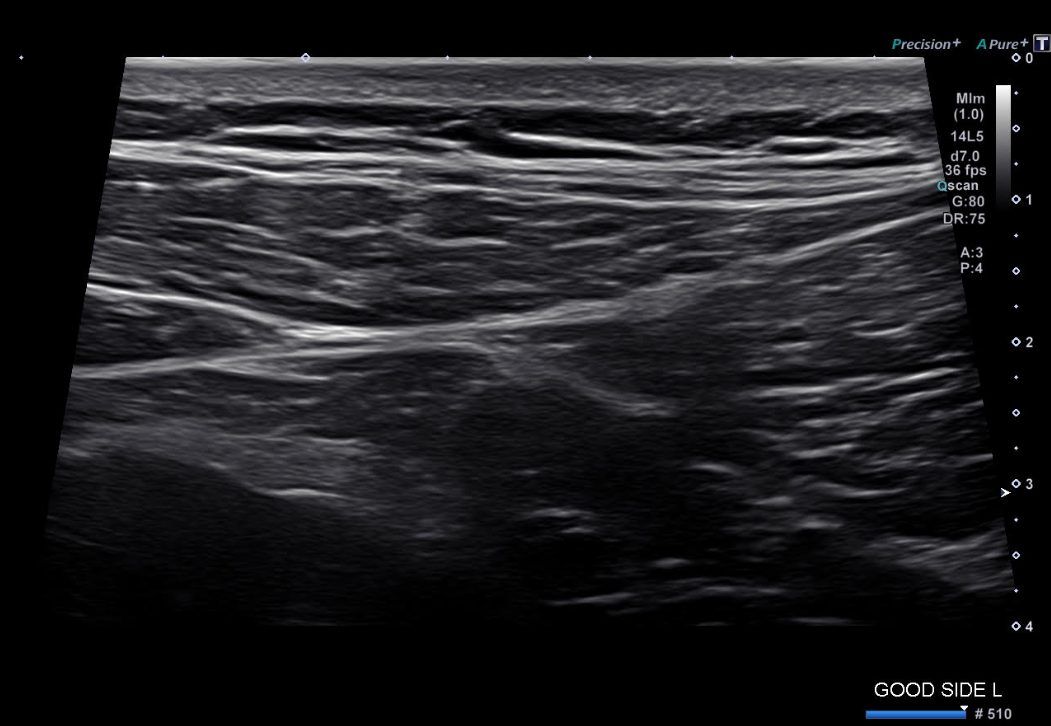
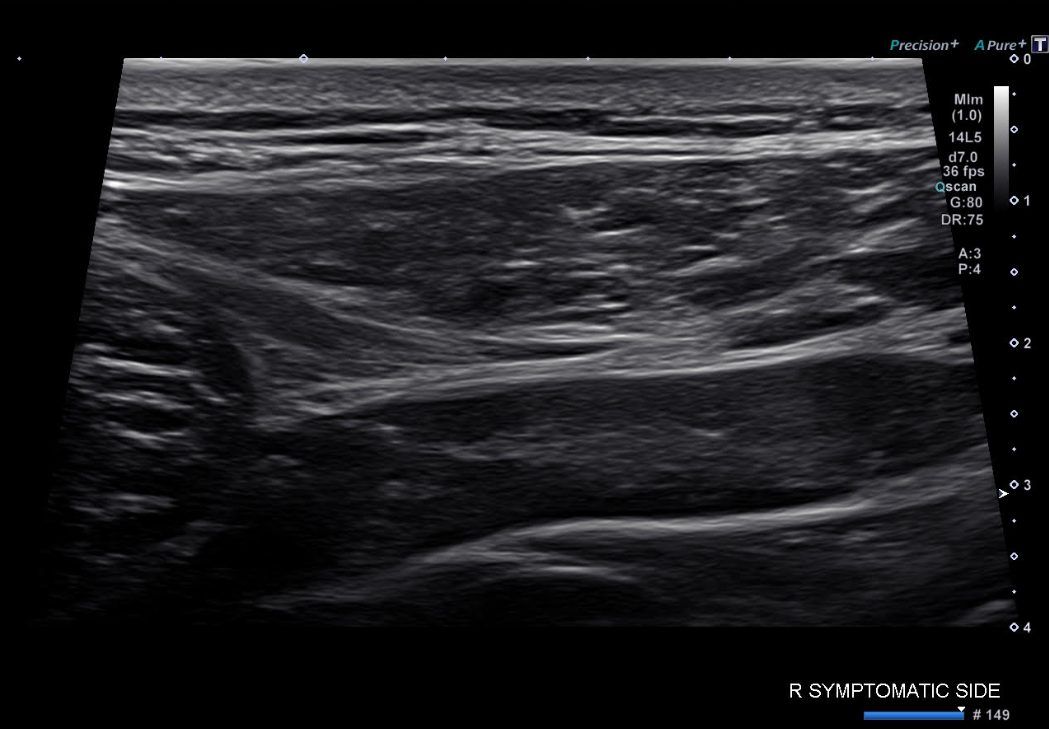
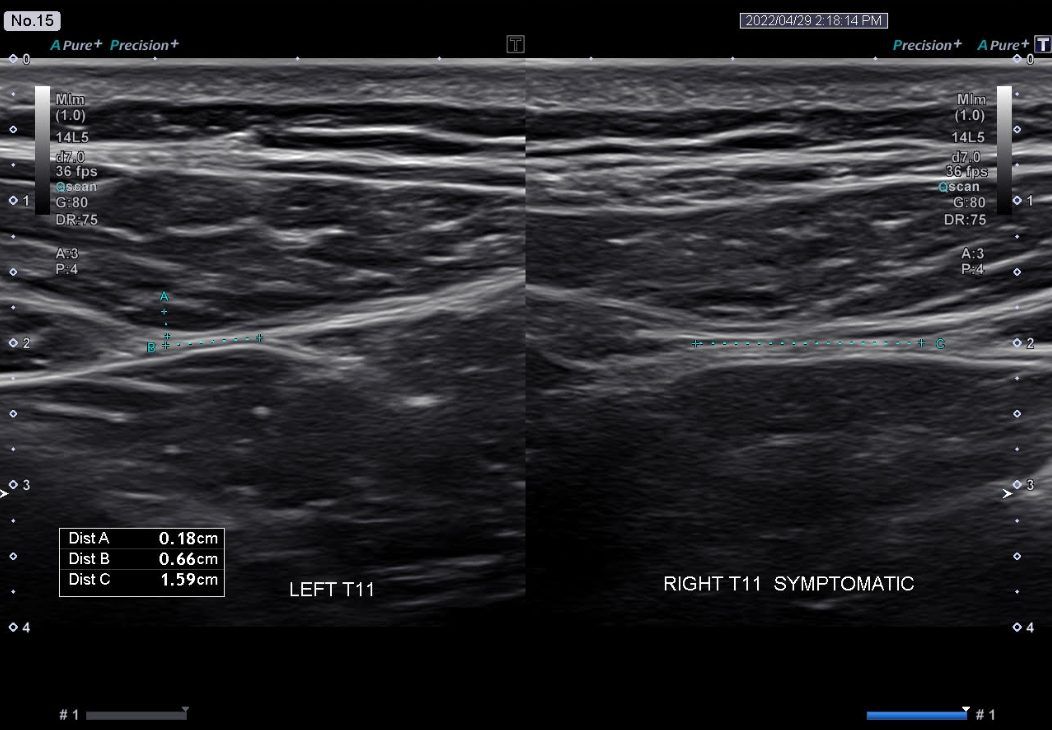
Physical palpation revealed subtle densification along the lateral raphe region – a complex of dense connective tissue formed by the fusion of layers of the thoracolumbar fascia (TLF). The TLF is often described as a “fascial zipper” along both sides of the lower back whose dysfunction gives a sensation of “disconnect” rather than pain.

After six weeks of multimodal treatment, the athlete reported improved abdominal wall activation, decreased compensatory lumbar pain, and restored efficiency of rotational action and sprint mechanics.
Lateral raphe tears are common in athletes, often formed by repetitive microtraumas that worsen over time. In this case, we suspect that the raphe failed due to a sudden rotational load during soccer that may have created the initial tear, aggravated by TLF densifications that disrupted load transmission.
Raphe tears rarely present as localized pain at the site of injury. Instead, tensegrity of the abdominal canister is destabilized, and the athlete loses a reflexive co-contraction between the anterior and posterior stabilizers.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















