Patients with EDS/hypermobility spectrum disorders are particularly susceptible to shoulder dysfunction due to the shoulder’s unique ball-and-socket architecture. Standard tests and imaging rarely provide sufficient information to recommend specific interventions. This case study demonstrates how multimodal functional testing that includes dynamic ultrasound imaging and ShowMotion kinematic analysis provides superior results that help form the basis for personalized treatment.
The patient presented with chronic pain in the neck, upper back, and scapular region. There was no history of prior trauma, but the patient had a high hypermobility score.
After testing for general joint hypermobility, we used additional assessments for shoulder-specific functionality:
We scanned the glenohumeral joint and found gapping of the anterior joint space, but no translation or indication of labral tearing. We found fraying and instability of the latissimus dorsi and serratus anterior fascial insertions, with possible fascial decoupling.
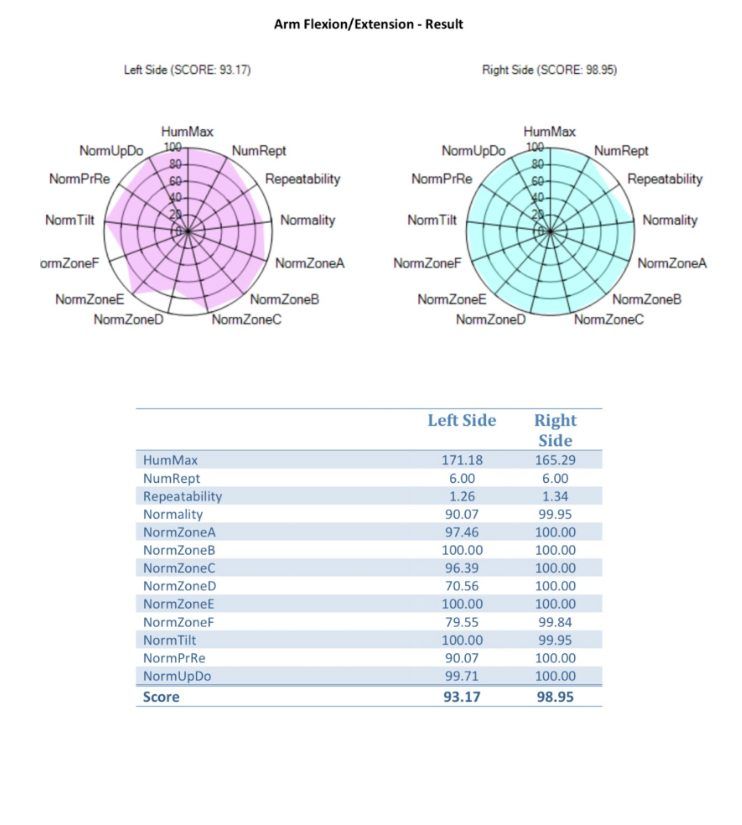
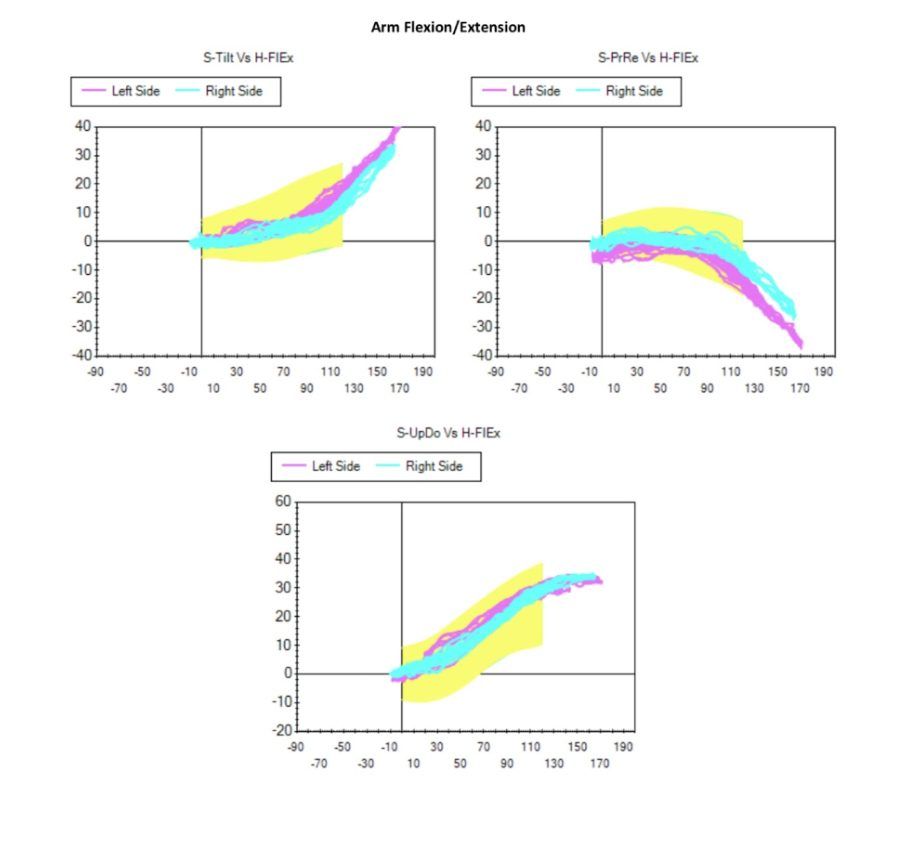
ShowMotion is an objective tool for joint movement analysis that uses motion tracking sensors, placed on the patient’s skin to collect data about movement quality.
Our ShowMotion analysis revealed:
This case called for a rehab-first strategy to restore the competency of the patient’s neuromotor control system before introducing any structural biologic support. Prolotherapy and orthobiologics may be introduced after coordinated neuromuscular pathways have been restored.
In patients with hypermobility spectrum disorders presenting with upper quadrant pain, standard orthopedic and imaging protocols are insufficient to inform a comprehensive treatment approach.
Our case emphasized:
Augmenting standardized tests with dynamic ultrasonography and data-rich objective feedback from ShowMotion gave us an objective basis for intervention planning, dramatically improving the patient’s odds of satisfactory treatment.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















