Typically, MRI is the imaging modality of choice for hip labrum issues. But can hip labral detachment be detected with high-resolution ultrasound? The answer is yes, in certain cases, under specific circumstances.
I have been scanning hips for years, and one thing that still amazes me is how much dynamic ultrasound can reveal when we take the time to look beyond static images.
Not everything in the hip is obvious. Some findings are subtle, mechanical, and only show themselves during dynamic imaging, where the joint is moving.
In fact, there are several key factors that MRI cannot detect, such as:
These are all movement-based factors that can only be identified with dynamic imaging. During MRI, the patient is required to lie still as images are collected of the problematic region. However, static images do not show how the body’s structures interact, and that information can be critical for diagnosing musculoskeletal disorders.
Meanwhile, in the hands of a skilled practitioner, high-resolution ultrasound imaging can reveal:
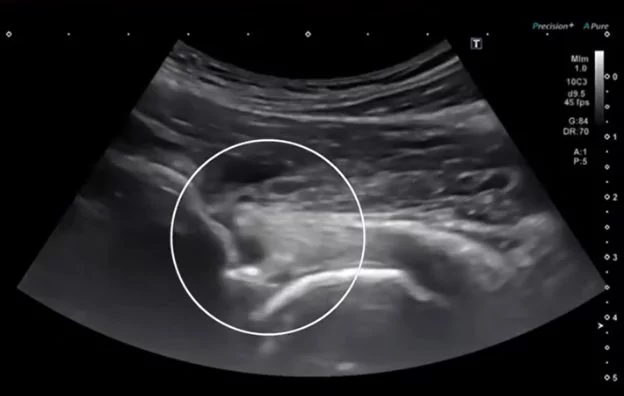
For example, during pressure or rotation, we may see a burst of synovial fluid moving through a separation plane at the chondrolabral junction.This is a strong dynamic indicator of an anterior labral detachment or a suction-seal failure.
This is something that MRI is not designed to show — and honestly, it’s deeply satisfying when the dynamic exam explains the patient’s symptoms better than static imaging.
While ultrasound cannot describe a labral tear as well as an MR arthrogram, in real clinical practice, dynamic imaging gives us immediate information we can use to diagnose and treat hip labral dysfunction.
Dynamic ultrasound does not completely replace MRI, but it can quickly fill in functional gaps that MRI cannot detect. For this reason, diagnostic ultrasonography is one of the most powerful tools we have in our clinical practice. The ability to dynamically observe the body’s structures in real time gives us tremendous insight into the underlying mechanisms of pain and dysfunction, helping to expedite the patient’s recovery.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















