March 28, 2026

Proximal Hamstring Tendinopathy (PHT), sometimes called high hamstring tendinopathy, is a condition involving the upper hamstrings where they attach to the ischial tuberosity – aka sitbones – at the base of the pelvis. PHT is a common sports injury associated with repetitive overuse, but it can also affect sedentary non-athletes, often from excessive sitting or driving.
Learn about PHT, its symptoms and causes, and advanced treatment methods that are changing the way proximal hamstring tendinopathy is diagnosed and treated.
Proximal hamstring tendinopathy is a type of insertional tendinopathy – irritation at the site where hamstring tendons attach to the sit bones. PHT is a chronic overuse condition, not an acute tear or strain. It is marked by irritation, degeneration, or micro-tearing of the hamstring tendons where they attach to the ischial tuberosity.
While PHT commonly affects athletes and runners, it can also affect sedentary populations, where it is typically associated with compression from excessive sitting. Other non-athletic factors include older age, poor flexibility, and obesity.
Symptoms of proximal hamstring tendinopathy include:
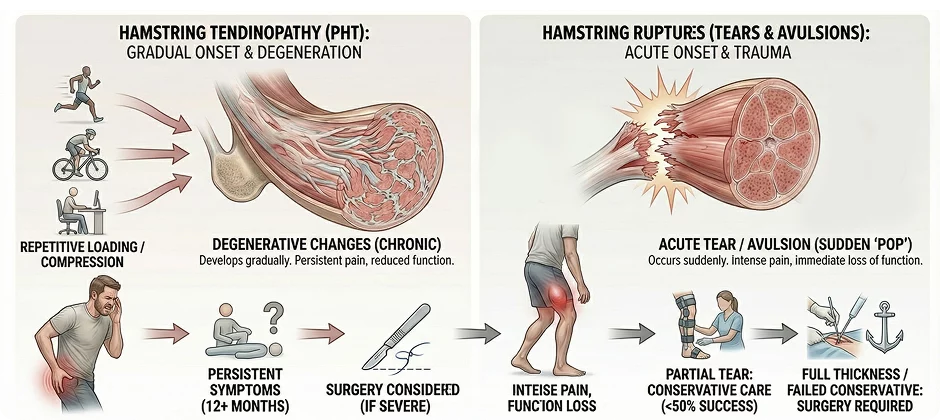
Unlike acute hamstring strains, tears, or avulsions that occur suddenly, PHT develops gradually from repetitive mechanical loading or compression. Tendinopathies often develop during activities like kicking or sprinting, with players often reporting a sudden popping sensation followed by intense pain, While PHT is most common in sprinters and distance runners, it can also affect cyclists, dancers, rowers, and sedentary people who sit for long periods, or who suddenly increase their physical activities.
PHT can lead to degenerative changes in the tendon tissue, resulting in persistent pain and reduced function that hampers physical performance. If left untreated, hamstring tendon degeneration can lead to tears or ruptures, compounding the problem, and requiring more invasive treatment.
While a partial thickness tear of the proximal hamstring tendon may be treatable via conservative methods, the success rate is less than 50%. Full thickness tears and partial tears that do not respond to conservative care may require surgery.
PHT surgery may be indicated when symptoms persist for 12+ months and severely impact athletic performance or quality of life.
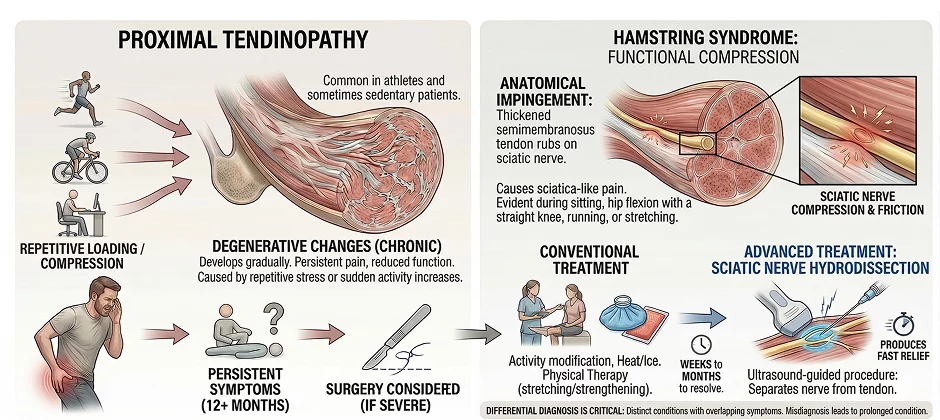
Hamstring syndrome is a less common condition that causes pain in the buttocks, often mimicking symptoms of proximal tendinopathy. Hamstring syndrome is most common in athletes, although it sometimes appears in sedentary patients. It can arise from repetitive stress from sports or exercise, or from sudden increases in physical activity.
Hamstring syndrome occurs when the thickened semimembranosus portion of the proximal hamstring tendon begins to rub against the sciatic nerve, causing friction and pain that is sometimes mistaken for sciatica. Pain from hamstring syndrome is especially evident during sitting, hip flexion with a straight knee, running, or stretching.
While hamstring syndrome, proximal hamstring tendinopathy, and sciatica share overlapping symptoms, they are all distinct conditions requiring different treatment approaches. During the initial diagnostic exam, clinicians must take care to differentiate the three, since misdiagnosis can lead to inappropriate treatment, prolonging or even worsening the patient’s condition.
Conventional treatment for hamstring syndrome typically involves activity modification, applying heat and ice to manage pain, and physical therapy aimed at stretching and strengthening the hamstring muscles. However, this approach can take from weeks to months to resolve the condition. Ultrasound-guided sciatic nerve hydrodissection is an advanced treatment that produces fast relief by enabling the sciatic nerve to glide without friction.
Unlike tendon tears, ruptures and avulsions that are categorized by type and severity, tendinopathies are typically categorized by which tendon is primarily affected, the severity or chronicity of the injury, and its stage of pathological progression. The proximal hamstring has three tendons – the semitendinosus, the long head of the biceps femoris, and the semimembranosus. Of the three, the semimembranosus is the most commonly affected by PHT.
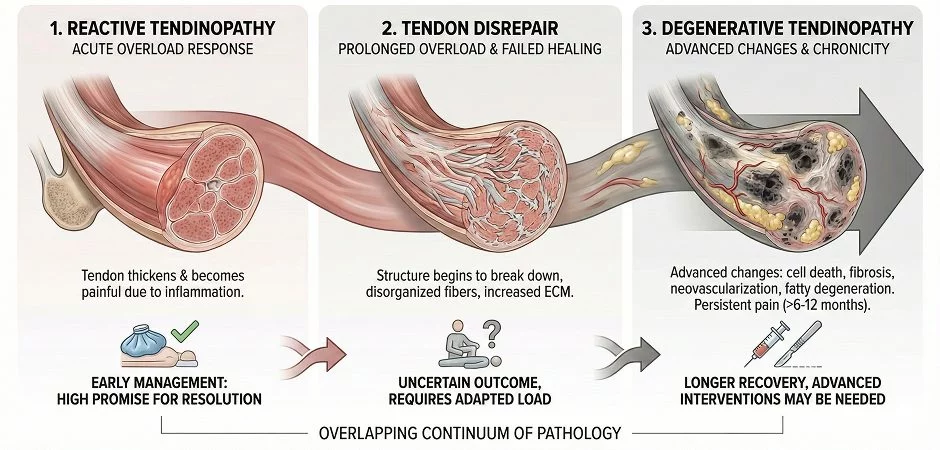
The Tendinopathy Continuum Model is the most common framework for categorizing PHT. Although the model describes three distinct stages, it is important to note that tendon pathology occurs on an overlapping continuum.
Stages of PHT based on the Tendinopathy Continuum Model are:
When considering the causes of PHT, it is important to recognise that the body’s structures do not function in a vacuum – they work interdependently, and pathology in one area can cause, and be caused by, issues in another. Even highly trained athletes can neglect critical factors that increase their injury risk. One key factor is the importance of overall pelvic stability, which is highly influenced by the sacroiliac (SI) ligaments.
The sacroiliac (SI) joint and its ligaments are central to pelvic stability, connecting the base of the spine to the pelvic bones, and helping to transfer loads between the spine and lower extremities. Because the proximal hamstrings attach directly to the ischial tuberosity of the pelvis, any disruption in pelvic mechanics can increase mechanical stress on the hamstring tendons. SIJ instability often involves compression or entrapment of the Posterior Femoral Cutaneous Nerve (PFCN) and/or the sciatic nerve, mimicking symptoms or coexisting with PHT.
SIJ instability often involves compression or entrapment of the Posterior Femoral Cutaneous Nerve (PFCN) and/or the sciatic nerve, mimicking symptoms of – or coexisting with – PHT. While the two conditions can occur simultaneously, PFCN entrapment can happen without hamstring involvement.
The sacrotuberous ligament can also play a role in pelvic stability and hamstring function. The ligament forms a functional bridge between the proximal hamstring muscles and the SI joint. Repetitive overloading of the hamstrings can lead to loss of continuity between those structures, disrupting tensegrity and reducing performance.
The hamstrings help to regulate pelvic position and load transfer, and tight or overactive hamstrings can increase SI joint tension, affecting pelvic dynamic stability. In addition, weak core and/or gluteal muscles, or tight hip flexors, can increase load on the proximal hamstrings, causing chronic irritation at the tendon-bone junction.
Because SI joint dysfunction shares symptoms with PHT, misdiagnosis is common. To promote full recovery and optimize function, a holistic diagnostic approach is critical.
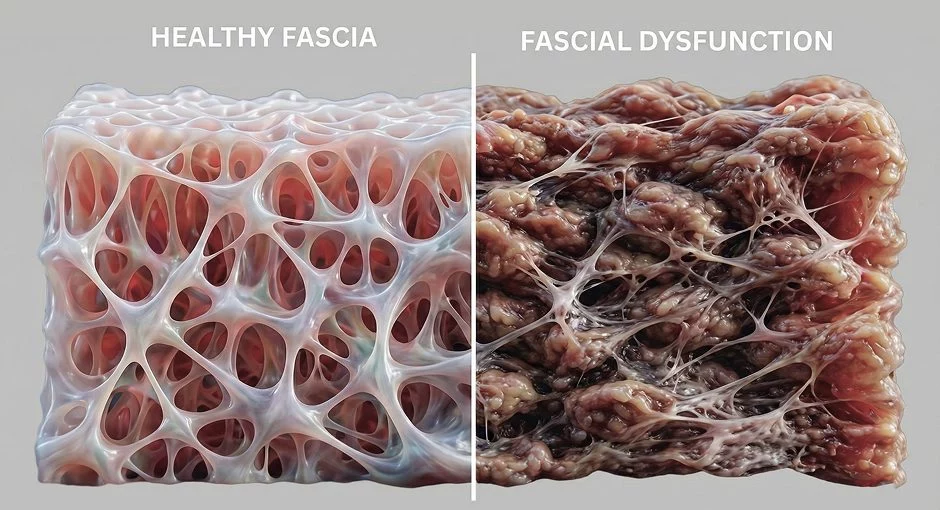
Fascia is a collagenous network of tough, elastic connective tissue that surrounds, supports, and interconnects muscles, tendons, nerves, and other structures. While collagen is its dominant component, fascia is highly embedded with hyaluronic acid and water molecules that form a slippery gel, reducing friction between the body’s structures and allowing for gliding of nerves and blood vessels. Fascia works with muscle to guide and control movement, and to distribute forces during physical activity.
Fascia works with muscle to guide and control movement, and to distribute forces during physical activity. At the same time, the myofascial system creates elastic tension that holds the body’s structures in place during movement – a concept called tensegrity. When tensegrity is compromised, coordinated muscle recruitment is disrupted, creating inefficient movement patterns with the potential to cause injury.
Fascial dysfunction refers to restrictions, adhesions, or thickening of fascial layers, interfering with muscle action and disrupting load transfer. Fascial dysfunction can be a significant contributing factor in proximal hamstring tendinopathy, altering biomechanics, increasing tension on the proximal hamstring tendons, and restricting tissue gliding. Nerves and blood vessels can become entrapped in densified fascia, causing pain and creating compensatory movement patterns that overload the tendons.
When the hamstring muscles cannot glide, the gluteal muscles may be prevented from firing, creating overload on the hamstring tendons. Failure to recognize the importance of fascia in PHT treatment can undermine your rehabilitation protocol and prolong your recovery. Fascial manipulation therapy can help to restore the functional properties of fascia, liberate entrapped nerves and blood vessels, and promote performance recovery.
When it comes to diagnosis, proximal hamstring tendinopathy can present challenges. Because PHT develops gradually, its onset and progression can be difficult to pinpoint.
Key diagnostic challenges include:
Even with magnetic resonance imaging (MRI), diagnosis can be difficult. MRI can show tendon thickening and edema at the ischial tuberosity, but it has a high rate of false positives and is not a reliable imaging source when used in isolation. By contrast, high-resolution ultrasonography may provide more definitive results.
Researchers have recently developed new criteria for ultrasound imaging based on the Tendinopathy Continuum Model. This development represents a quantum leap forward in diagnostic imaging, based on stages of PHT progression. The research team found intra-rater and inter-rater reliability to be “substantial to almost perfect” in diagnosing tendinopathy.
In general, accurate diagnosis of movement-based pathologies requires dynamic imaging. When combined with clinical results, dynamic high-resolution ultrasound can dramatically improve diagnostic accuracy, differentiating PHT from other conditions, while simultaneously identifying coexisting pathologies.
Conventional PHT treatment typically involves activity modification, load management, and pain relief for initial symptoms and flare-ups. As healing progresses, physical therapy and progressive rehabilitation exercises are added to restore function. With conventional treatment, recovery time can take from one to three months for uncomplicated cases, and longer for chronic cases. Progression and consistency are key factors in restoring pain-free function.
In today’s integrative medicine space, new approaches and technologies are transforming the way PHT is diagnosed and treated.
High Resolution Diagnostic Ultrasonography
High-resolution ultrasonography enables clinicians to dynamically observe the proximal hamstrings and their tendons in real time, providing insight into their interactions with adjacent structures. Factors like SIJ and fascial dysfunction, pelvic instability, and tendon degeneration can be visualized in the same session. Capabilities for sonoelastography and superb microvascular imaging allow for in-depth assessment of the stages of PHT degeneration.
Extracorporeal Shockwave Therapy (ESWT)
ESWT uses high-speed acoustic waves to reduce pain and inflammation, and to stimulate healing of stubborn tendons at the cellular level, dramatically accelerating the recovery process.
High Intensity Laser Therapy (HILT)
High Intensity Laser Therapy (HILT) is a non-invasive treatment that uses high-power light energy to reduce pain and inflammation, and accelerate tissue repair. A 2022 randomized study sought to establish the effectiveness of HILT in treating proximal hamstring tendinopathy in athletes. They found that athletes treated with HILT for three weeks had significantly lower pain scores than those given conventional treatment alone.



Dry needling targets myofascial trigger points – tightly contracted nodules of muscle fibers that cause pain and limit muscle action. Trigger points are frequently present in overuse injuries. The procedure involves insertion of non-medicated (dry), filament-thin needles into the nodules under ultrasound guidance, eliciting a relaxation response.
Platelet Rich Plasma (PRP)
PRP uses a high concentration of platelets, extracted from the patient’s own blood. When injected into damaged tendons under ultrasound guidance, PRP delivers stem cells and growth factors that promote and accelerate tissue healing.
Targeted Physiotherapy
Physical therapy for PHT should be personalized to target factors specific to the individual patient. Weak gluteal muscles, tight hip flexors, SIJ dysfunction, and pelvic instability are all variables that should be considered when crafting a customized protocol.



While non-athletic patients may only require baseline functional mobility, athletes need a more structured rehabilitation program involving progressive overload and sport-specific actions. Sports rehab protocols may include plyometric training, sprint progressions, exercises for lumbopelvic stability, and strengthening exercises for gluteal and hamstring muscles. Biomechanical deficiencies in the lower kinetic chain should be identified and addressed.
Chronic overuse injuries like PHT have a gradual onset, growing more painful over time until symptoms can no longer be ignored. Early intervention can prevent tendon degeneration, but many delay treatment in hopes of the condition self-resolving. Medical doctors often misdiagnose PHT due to its fairly new discovery and shared symptoms with other pathologies.
At NYDNRehab, our holistic, personalized approach to PHT is backed by 20+ years of hands-on clinical experience. Our clinic features some of the most advanced technologies available in integrative medicine, including the highest resolution ultrasound available. Our expertise in sports rehabilitation has helped countless athletes return to play at pre-injury performance levels, with reduced risk of re-injury.
For accurate diagnosis, accelerated healing, and rapid recovery from proximal hamstring tendinopathy, without drugs or surgery, contact NYDNRehab today.
Request an appointment»
![]()
Our location: 11 West 25th Street 5th floor, New York, NY 10010

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































