March 16, 2026

Tailbone pain, clinically called coccydynia, describes pain and discomfort surrounding your coccyx – the small triangular bone at the base of your spinal column. Acute pain can arise after a fall on your bottom, often involving a coccyx bruise or fracture, or it can develop gradually from certain conditions and activities.
We answer your questions about the coccyx, the various causes of pain, and new advanced treatment strategies that reduce coccyx pain and inflammation and accelerate healing.
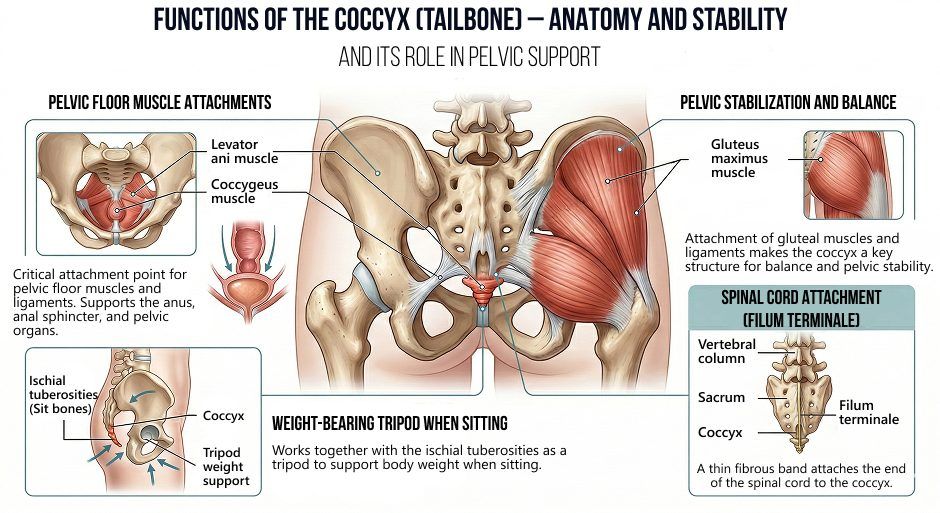
The coccyx (aka tailbone) serves as a critical attachment point for your pelvic floor muscles and ligaments, providing an anchor that supports the anus, anal sphincter, and pelvic organs. Its connections to the gluteus maximus and levator ani muscles make the coccyx a key structure for balance and pelvic stability. It also works together with the sit bones, acting as a weight-bearing tripod that supports the body when sitting. A fibrous band called the filum terminale attaches the spinal cord to the coccyx.
Coccyx pain typically arises from either trauma, pressure or overuse, although in rare cases it can arise from a tumor or infection.
Common causes of coccyx pain include:
Coccygodynia is relatively rare, estimated to comprise only 1–3% of all back pain disorders. The condition most frequently occurs in adult females and obese individuals
Fascia is a body-wide web of thin, elastic connective tissue that envelops and connects muscles, bones, ligaments, nerves, blood vessels, and organs throughout the body. It is made up of collagen, embedded with sensory nerves, and infused with hyaluronic acid, making it slippery, and enabling the body’s structures to glide without friction.
Fascia provides structural support to the pelvic floor by maintaining balanced elastic tension – a phenomenon known as biotensegrity – that holds structures in place as you move. Fascia surrounds the coccyx segments, and the coccyx is linked to broader fascial networks, creating a chain of tension from the lower back, hips, abdomen and even lower extremities.
Fascial connections establish the coccyx as an anchor for the pelvic floor and posterior pelvic structures. When fascial planes become dysfunctional, pelvic tension is disrupted, and the coccyx may be subjected to excessive loads, causing pain. Nerve may also be entrapped in densified fascia, generating pain.
While tailbone pain often self-resolves, severe pain that does not get better after a few weeks may indicate more serious issues that require medical attention.
To accurately diagnose and treat coccydynia, the exact underlying cause of pain must be identified. Coccydynia diagnosis relies heavily on health history (to determine onset and review symptoms), and a physical exam, to inspect the area for swelling or bruising, reproduce the pain by applying pressure, assess coccyx mobility, and evaluate pelvic floor function. Posture, hip and spine range of motion, and abnormal movements are taken into account.
Imaging with xray or MRI often comes back normal, despite pain symptoms, and is typically reserved for severe cases, or when there is a history of significant trauma.
Treatment typically begins with conservative care. Applying ice can help to numb pain and reduce inflammation, and use of a cushion when sitting can help to reduce pain. Avoid excessive sitting, and substitute activities like rowing or cycling with alternatives like walking or swimming.
Modification of lifestyle factors like poor posture and excess body weight can help relieve symptoms over time. Dietary changes can help reduce straining during bowel movements. Eliminate sugary foods and beverages and limit foods like pasta and rice. Steer clear of fast and ultra-processed foods. Eat mostly fresh fruits and vegetables, pastured meats, wild caught fish, and fermented foods like sauerkrauts, kimchi, kombucha, and cultured dairy.
Conservative treatment interventions include:








In severe, persistent cases, a coccygectomy – a surgical procedure that completely removes the coccyx – may be recommended. However, success rates can vary, and removing the coccyx can dramatically affect functional mechanics of the lumbopelvic region.
You can significantly reduce your risk of coccydynia by taking common-sense steps that improve your overall health.
Conservative treatment interventions include:






Tailbone pain can range from uncomfortable to debilitating, but you don’t have to deal with it on your own. At NYDNRehab, we leverage the most advanced holistic treatment approaches to eliminate coccydynia pain and accelerate recovery. We use the highest-resolution ultrasound to guide our energy therapies and injection procedures, ensuring precise and effective treatment.
Our personalized one-on-one physical therapy sessions are focused on treating the whole patient, not just your symptoms, providing effective and lasting relief, without drugs or surgery. Contact NYDNRehab today, and get rid of tailbone pain so you can get back to doing the things you love!
Request an appointment»
![]()
Our location: 11 West 25th Street 5th floor, New York, NY 10010

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































