February 23, 2026
Back pain is one of the most frequently reported complaints among adults, affecting nearly 70 million Americans, with 8% reporting chronic persistent pain that restricts their daily activities. Back pain accounts for over $12 billion in medical expenses per year, and adults with back pain are more likely to use medical services. Additional costs include lost work days, reduced productivity, diminished overall health, and feelings of depression and anxiety.
According to a report by GWU’s Health Policy Institute, patients who seek alternative care for back pain instead of conventional medical care report a higher level of satisfaction with their care, noting that alternative providers are more likely to explain their treatment and provide advice on self-care. Now, integrative practitioners have new regenerative tools at their fingertips that are transforming the way back pain is treated.
Learn about the types and causes of back pain, new inroads in back pain research, and how regenerative energy technologies and biologic therapies are revolutionizing back pain treatment and restoring pain-free mobility.
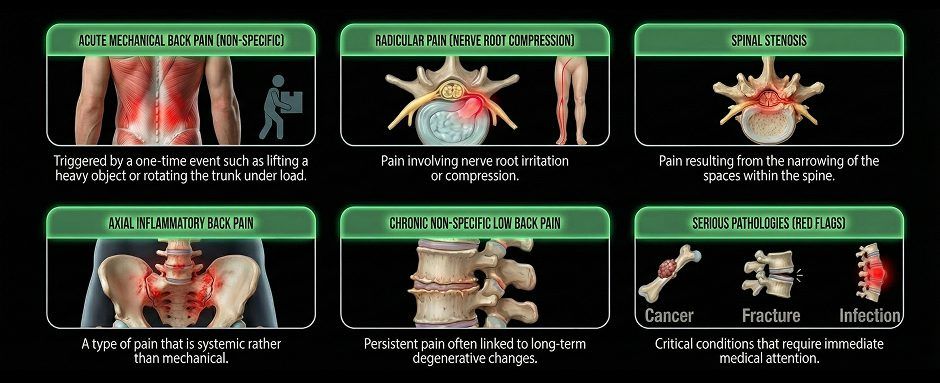
Despite its widespread prevalence, only 2-4% of back pain is due to serious pathology such as cancer, infection or fracture. Over 90% is mechanical in nature, meaning it is caused by some type of motor or metabolic dysfunction that can be improved or completely corrected via conservative, non-surgical treatment.
Common types and causes of back pain include:









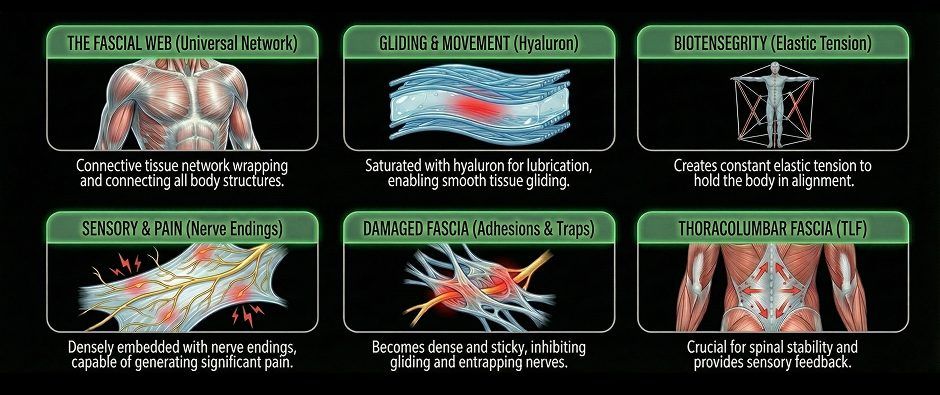
Fascia is a universal network of connective tissue that wraps and connects tissues and structures throughout the body. Fascia coordinates with muscle to guide and control movement, distribute forces, enable gliding among various structures, and hold vital organs in place during movement. The functional role of fascia in human movement has only recently been recognized, sparking a vast body of research into its function and mechanisms.
Fascia is a collagenous tissue saturated with hyaluron – a gel-like substance that lubricates the tissue and makes it slippery, allowing for tissues and neurovascular bodies to glide smoothly without friction. Fascia is tough, smooth, and elastic, creating a state of constant elastic tension called biotensegrity that holds your body in alignment. Fascia is also densely embedded with sensory nerve endings, capable of generating more pain than muscle tissue.
When damaged, fascia becomes dense and sticky, losing its functional properties, adhering to other structures, and inhibiting gliding. Nerves can become entrapped by densified fascia, causing significant pain. Damaged fascia interferes with muscle action, impairing mobility and causing structural misalignment. It may develop myofascial trigger point – hard knots of tightly contracted fibers that cause pain and impede performance.
The thoracolumbar fascia (TLF) plays a significant role in spinal stability and mobility. The TLF helps to transmit external loads from the spine to the pelvis and lower extremities. It is densely embedded with mechanoreceptors that send important information to the brain about spinal position, allowing for corrections to optimize structural spinal support.
The increased thickness of the TLF corresponded to greater pain intensity, while atrophy of the lumbar multifidus muscle was linked to decreased lumbar flexion. The authors concluded that treatment of chronic low back pain should target not just muscle, but fascial components as well.
The research team’s conclusion suggested that TLF thickness correlates with altered fascial remodelling in chronic LBP subjects, resulting in a “frozen back”.
There are dozens more studies like these that point to fascia as a key player in chronic low back pain. Yet many medical doctors are unaware of fascia’s properties or its role in musculoskeletal dysfunction. By overlooking this important factor, patients are often subjected to treatment that merely masks symptoms, while failing to address their underlying cause.
Radicular back pain generated from a compressed nerve root is most often caused by a herniated disc, but not always. The transforaminal ligaments are small, fibrous bands of connective tissue, commonly found in the lumbar spine, that span the intervertebral foramen – the space through which the nerve roots exit the spinal canal.
The transforaminal ligaments cross directly in front of the nerve root as it exits, and in some cases they can entrap or compress the exiting nerve, causing significant pain. Because back pain caused by ligaments is relatively rare, doctors may not even consider their contribution to back pain. Many doctors are unfamiliar with this phenomenon, but the ligaments should be considered after more common causes have been ruled out.
The causes of chronic back pain can be multifaceted, and it can be challenging to single out a specific cause based on symptoms alone. Medical doctors may refer patients for MRI if initial treatment strategies fail to alleviate pain. But MRI is costly, inconvenient, and uncomfortable for the patient, and results often come back negative, with no evidence of mechanical issues as a source of back pain.
High resolution ultrasonography provides a safe, cost-effective and convenient imaging alternative to MRI, with minimal discomfort for the patient.

MRI has long been considered the gold standard for spinal imaging, and it still has its place in specific circumstances, but ultrasound is gaining ground as the imaging modality of choice for back pain diagnosis.
The following table compares MRI and Ultrasound for back pain imaging:
In the past, back pain was typically treated with bedrest, muscle relaxants, and anti-inflammatory drugs. In persistent cases, patients were often treated with opioids, which led to a catastrophic addiction crisis among back pain patients. But in recent years, treatment has evolved.
Today, conventional medical treatment includes patient education and encourages moderate physical activity. Physical therapy exercises and manual therapy are often recommended in the early stages, with the use of NSAIDs for pain and inflammation. However, medical doctors focus mostly on pain management, and do not consider the involvement of structures outside of the locus of pain.
By contrast, integrative practitioners consider the whole patient, not just their symptoms. Mechanical back pain often has its origins in structures outside the radius of pain, and accurate diagnosis requires an in-depth understanding of human anatomy and biomechanics. Instead of focusing on pain management, integrative clinicians pursue a holistic path to unearth the true source of pain and correct it.
Rather than relying on synthetic drugs and surgical mechanical fixes, regenerative therapists tap into the body’s innate self-healing mechanisms. Cartilagenous tissues like ligaments, tendons and fascia often have low vascularity, making them slow to heal.
Regenerative therapies give avascular tissues a boost by stimulating the body’s own immune response, to attract stem cells and growth factors to the treatment site, dramatically accelerating the healing process.
Platelet Rich Plasma (PRP)
PRP therapy uses a sample of the patient’s own whole blood, spun in a centrifuge to extract a high concentration of platelets. When injected into damaged tissues, PRP initiates tissue repair by releasing biologically active agents. To be effective, it is critical to use the correct concentration and quality of platelets, and to and follow proper isolation techniques.
Prolotherapy
Prolotherapy uses a biologically neutral solution to irritate stubborn tissues, triggering the body’s innate healing mechanisms to grow new normal tendon, ligament and muscle fibers. Prolotherapy is often used for slow-to-heal tendon and ligament ruptures, where low vascularity inhibits tissue healing.
Hyaluronic Acid Injections
Hyaluronic acid (HA) is a natural component of joint synovial fluid and fascial tissue. When combined with myofascial release techniques, hyaluronic acid injections can help to rehydrate fascial tissue and revitalize its functional properties. HA also supports healing by replenishing joint synovial fluid.
Interfascial Plane and Nerve Hydrodissection
The hydrodissection procedure injects a saline solution into densified fascial layers under ultrasound guidance, separating the layers and releasing entrapped nerves and blood vessels. Hydrodissection is often used in conjunction with manual fascial release and hyaluronic acid injections, to fully restore fascial integrity.




Multimodal Extracorporeal Shockwave Therapy (ESWT)
Extracorporeal shockwave therapy (ESWT) is a noninvasive treatment that uses high-energy acoustic waves to induce biological and physiological effects. ESWT reduces pain and inflammation, helps to realign and repair collagen fibers, promotes rehydration of synovial fluid and fascial tissues, and restores friction-free knee mechanics. ESWT is most effective when guided by high-resolution ultrasound imaging.
Extracorporeal Magnetic Transduction Therapy (EMTT)
EMTT transmits high energy magnetic pulses to targeted tissues that synchronize with the body’s own magnetic fields, triggering a regenerative response. EMTT waves can penetrate deep tissues to target difficult-to-reach tendons, muscles, bones and nerves.
TECAR Therapy
TECAR, an acronym for Transfer of Energy Capacitive and Resistive, is a non-invasive therapy that uses high-frequency electrical currents to deliver radiofrequency energy via a hand-held device, creating an electromagnetic field. TECAR triggers biological responses, including enhanced blood flow and oxygenation, increased cellular metabolism, improved lymphatic drainage, reduced inflammation, and pain relief.
PENS
Percutaneous neuromodulation (PENS) is a therapeutic approach that uses electrical stimuli to calm hypersensitized nerves, a common factor in chronic back pain. PENS involves the insertion of several filament-thin needles under ultrasound guidance into muscle tissue adjacent to the targeted nerve. PENS stimulates the nerve with varying waves of low-frequency electrical current to help restore optimal neural function.




The Stecco technique of fascial manipulation is a highly systematic approach that requires special training. When applied correctly to thickened fascial layers, Stecco not only restores elasticity and tissue gliding – it reactivates sensory receptors within the fascia, recalibrating the neuromuscular system and restoring efficient motor control.

This advanced methodology alleviates back pain, restores unrestricted movement, enhances physical performance, and optimizes whole-body mobility and stability. The Stecco Method was developed by Dr. Carla Stecco, the world’s leading specialist in fascial science.
Spinal mobility and stability is fundamental to all human movement, and good spinal alignment and function rely on strong, balanced muscles and connective tissues. Once your tissues are treated and ready to bear loads, a well-designed physical therapy program can set you up for long-term spinal health.
Steer clear of PT clinics that use generic treatment protocols in a group setting, and look for a rehabilitation center that offers one-on-one customized physical therapy.
New advanced therapies and technologies promise to revolutionize how back pain is diagnosed and treated, but they are rarely found under one roof, and many clinicians lack the training and expertise to effectively use them. Moreover, they do not provide stand-alone solutions, and are most effective when strategically used in combination with one another, and with manual and physical therapy.
The clinic at NYDNRehab in Midtown Manhattan is at the cutting edge of regenerative medicine, featuring a broad range of technologies and advanced therapies to effectively treat persistent back pain. Dr. Kalika’s experience and expertise is unrivaled, making NYDNRehab the clinic of choice for chronic back pain treatment in NYC.
Request an appointment »
![]()
Our location: 11 West 25th Street 5th floor, New York, NY 10010

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































