February 26, 2026

For millennia human physical culture has been admired and celebrated, with toned and sculpted bodies inspiring the world’s most revered artistic masterpieces, and highly trained athletes pitting strength against strength, providing entertainment for the masses in public arenas. But until recently, human musculature has taken all the credit.
Now, in the 21st Century, fascia has been cast into the spotlight, rising from obscurity as an insignificant wrapper for separating the body’s structures, and gaining recognition as a vital and dynamic tissue that not only holds everything together, but contributes substantially to mechanical force production and load distribution.
Discover new research about the mechanical properties of fascia, how it contributes to human movement, and how it factors into physical training, athletic performance, and injury prevention.
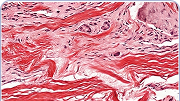
Fascia is an extensive network of thin, tough, elastic connective tissue that surrounds and connects structures and organs throughout your body. Once thought by scientists to be insignificant, fascia was typically stripped away and discarded during cadaver studies, leaving a gap in our understanding of human biomechanics.
Fascia is made up of about 90% type-1 collagen, giving it substantial tensile strength, and 10% elastin, giving it elastic properties. The tissue is richly embedded with hyaluronic acid, a polysaccharide found in joint synovial fluid, skin, and eyes. Hyaluranon has the capacity to attract and hold up to 1000 times its weight in water, forming a lubricating gel that allows fascia to glide without friction among other structures. Fascial tissue is also generously embedded with sensory nerves, making it a greater pain generator than muscle.
Some fun facts about fascia:
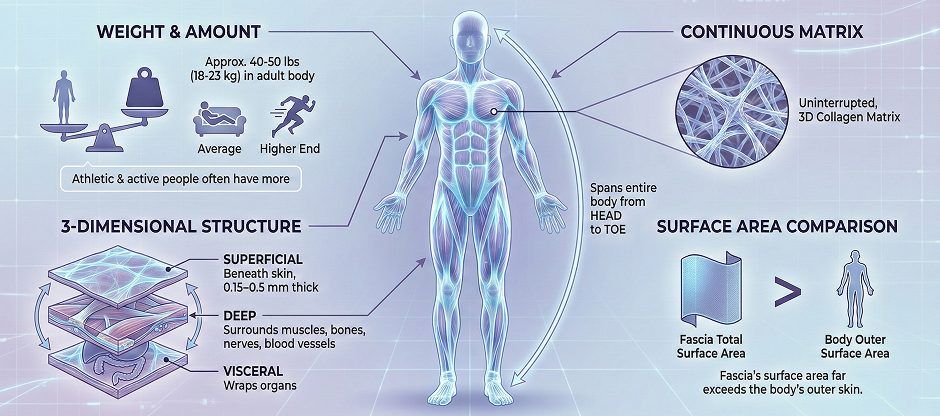
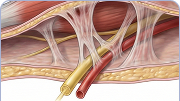
During movement, fascia holds organs and structures in place, facilitates frictionless movement of muscles, nerves and blood vessels, helps to guide and control movement, and participates in force production and load distribution. Fascia is fundamental to movement quality, providing elastic tension that preserves tissue integrity – a concept called biotensegrity.
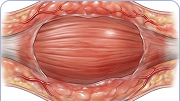
Until recently, fascia was regarded as a passive tissue whose only function was to envelop and connect other structures, such as muscles. But new research has redefined fascia as a dynamic tissue that works in coordination with muscle to facilitate movement. Fascia is able to transmit force across joints, store and release energy, and adapt to loading demands by becoming stronger and more resilient.
Fascia is made up of mostly type-1 collagen fibers, arranged in location-specific patterns. Collagen gives fascia its tensile strength, making it resistant to injury or overload from internal and external forces. Fascial tissue also contains a certain amount of elastin – a highly elastic fibrous protein that allows fascia to stretch and recoil back to its original shape. The collagen-to-elastin ratio varies, depending on the location and function of various fascial planes, but collagen is the dominant component.

Fascia is able to store and release elastic potential energy – think of stretching a rubber band and releasing it. The plantar fascia is a good example, storing energy and releasing it through various stages of the gait cycle – a phenomenon referred to as the windlass mechanism. Under the initial loading phase, the plantar fascia stretches, storing elastic energy, which It then releases at push-off as it returns to its original length, facilitating muscle in force production.
Fascia’s elastin content – and therefore its elastic properties – varies from one site to another, depending on its role in local mechanics. Elastic fibers are significantly more abundant in superficial fascia located directly beneath the skin than in deep fascia like the fascia latta, the tough band of fascia that runs along the outer thigh. Fascia’s ability to stretch and recoil is also dependent on its collagen fiber orientation. But elasticity is not fascia’s only contribution to biomechanics.
Although still in its early stages, current research suggests that fascia has active contractile capabilities. Unlike muscle contraction, which is driven by smooth muscle cells, fascial contraction is stimulated by specialized cells called myofibroblasts (MFBs). MFBs contain actin-myosin filaments similar to those in smooth muscle, enabling them to generate and sustain contractile force.
According to one recent study, MFBs actively regulate fascial tension, giving it the potential to impact musculoskeletal dynamics. The research team noted that MFB density varies from one fascial tissue to another, with greater density in the lumbar spinal fascia compared to the plantar fascia or fascia lata.
Fascia’s contractile capabilities may have strong implications for injury rehab, physical training and athletic performance, expanding and even redirecting the ways that myofascial dysfunction is approached and treated.
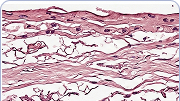
Contrary to traditional perceptions of fascia as a passive and insignificant tissue, we now know that fascia is one of the richest sensory organs in the human body, thanks to its vast surface area and high density of nerve endings. It is estimated that the entire fascial system boasts around 250 million nerve endings that primarily support sensory functions.
Sensory functions supported by fascia include:


Compared to skeletal muscle tissue, pain receptors (nociceptors) in fascia are notably denser, more sensitive, and more responsive to stimuli. Fascia’s free nerve endings have a lower mechanical activation threshold, meaning they respond to pain stimuli such as subtle deformations, shear, or stretch more quickly than muscle. Fascia nociceptors are especially sensitive to chemical irritation. Moreover, fascia-derived pain tends to be more diffuse, radiating, prolonged, and intense.
Under inflammatory conditions, fascia displays pronounced increases in nociceptor density, and hypersensitivity is sustained for a longer period of time. Fascia-generated pain has been linked to conditions like chronic low back pain, myofascial pain syndrome, and delayed-onset muscle soreness (DOMS).
When damage to fascial tissues leads to myofascial dysfunction, biotensegrity is compromised, resulting in inefficient biomechanics, reduced movement quality, reduced physical performance, and increased injury risk. Fascial tissue damage typically arises from alterations in the structure, mechanics, or biochemistry of fascia.
Such changes may include:
These alterations can impair fascial gliding, interrupt force transmission, impede proprioception, and contribute to pain, stiffness, and restricted mobility – all necessary components of quality physical performance.
When faced with musculoskeletal pain and injuries, the majority of conventional medical practitioners do not recognize fascia as a contributing factor, resulting in underdiagnosis, ineffective or insufficient treatment, and unsatisfactory patient outcomes. This is especially problematic for physically active patients who want to return to pre-injury performance levels.
Outside of orthodox medicine, holistic and integrative practitioners often have more extensive knowledge about the body’s fascial network, and how it impacts mobility and performance. They go beyond addressing only pain symptoms and structural damage at the site of injury, factoring in dysfunction along the entire kinetic chain, including fascial dysfunction. Holistic doctors typically steer clear of pain medications and reconstructive surgery, opting instead to treat the underlying causes of pain and dysfunction.
Holistic approaches to fascial injury, pain, and dysfunction include:




Traditional sports and fitness training focuses on building muscle size and strength, and enhancing sport-specific skills. Training regimens often center around muscle isolation exercises that target one muscle group at a time, along with cardiovascular conditioning and neuromuscular coordination. But without healthy fascia to help distribute forces, large and powerful muscles are useless for functional mobility.
Most sports-related overuse injuries occur when the body’s fascial planes are loaded beyond their functional capacity, and treatment interventions should include fascial therapy. Fascia responds to physical training by remodeling its collagen structure, making it stronger, more elastic, and more efficient at transmitting force loads.
Strong and healthy fascia is better able to handle high-intensity forces without injury from repetitive overload. Fascial mobility is enhanced by varied, multi-directional exercises that simultaneously recruit multiple body segments. Fascial training can take from 6 months to 2 years for optimal adaptation, and adaptations are specific to the load, speed, and direction of movement.





Functional mobility is strongly linked to overall health and quality of life, yet many people settle for sub-optimal movement, chronic aches and pains, and limitations on physical activity. Such physical disability is often caused, directly or indirectly, by fascial restrictions that undermine functional mobility. But fascial dysfunction is rarely a permanent condition, and in most cases it can be fixed with appropriate treatment.
At NYDNRehab, we treat the whole patient, not just your symptoms. We understand that the human body is more than the sum of its parts, and that pain in one area of the body is often caused by dysfunction elsewhere. Our clinic features the most advanced technologies and therapies for diagnosis and treatment currently available, backed by 20+ years of hands-on clinical experience and extensive training in rehabilitative medicine. Our personalized, one-on-one approach ensures that you get the best possible treatment, tailored to your specific needs.
You don’t have to settle for chronic pain and reduced mobility. Contact NYDNRehab today, and get moving again so you can live your life to its fullest.
Request an appointment »
![]()
Our location: 11 West 25th Street 5th floor, New York, NY 10010

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































