December 12, 2025

While knee OA has traditionally been considered a degenerative disease, advancements in regenerative medicine are breaking new ground, halting and even reversing cartilage erosion, and giving new hope to knee OA sufferers.
Knee OA involves more than just cartilage – It affects multiple tissues and structures, especially as the disease progresses. Early intervention is critical to slowing and reversing the degenerative process.
Tissues and structures affected by knee OA include:
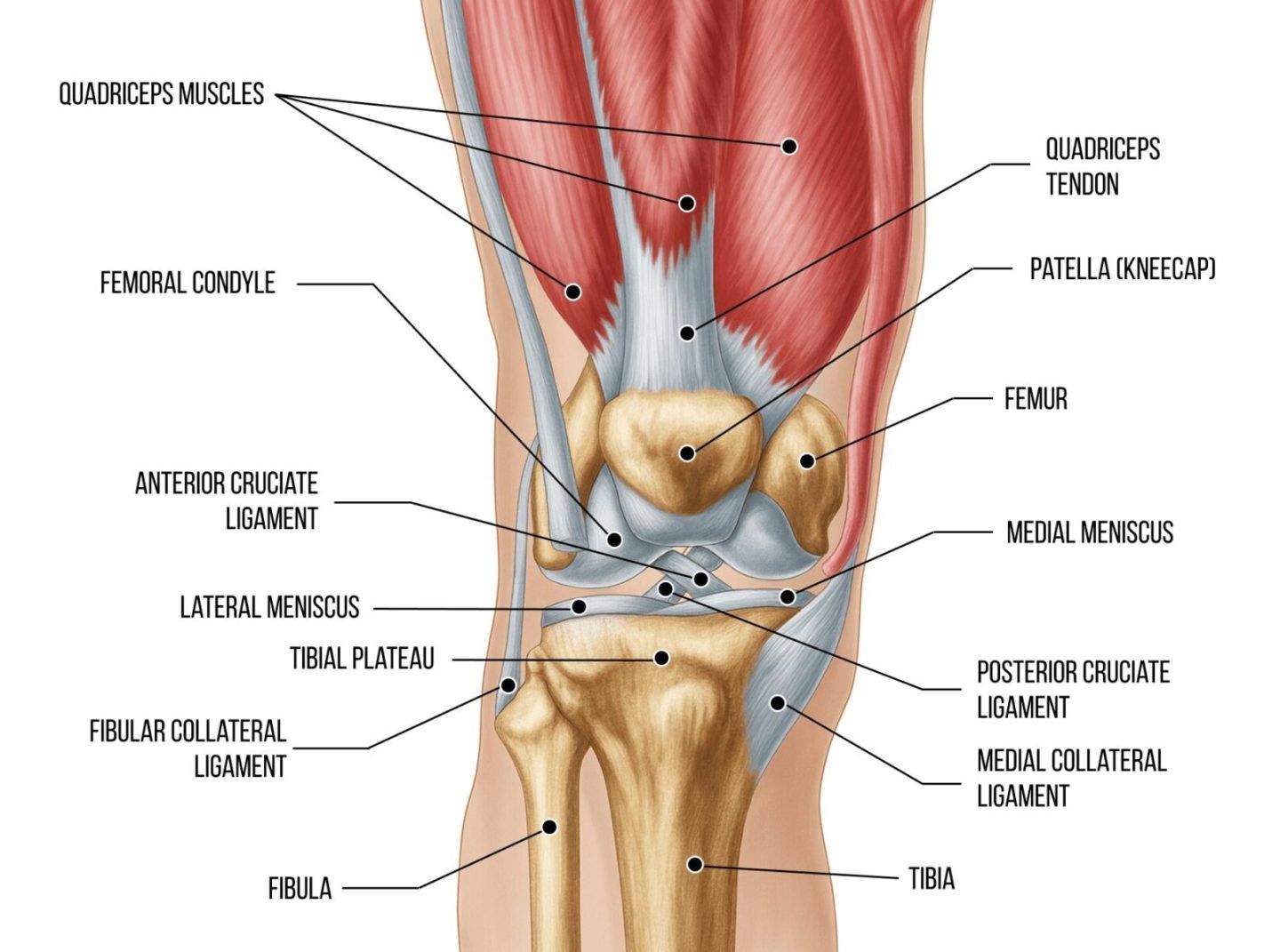
Managing pain and treating knee cartilage is not enough to resolve knee OA. The condition demands a holistic approach that addresses all affected structures, with the goal of strengthening and realigning the knee joint and restoring functional mobility.
Knee OA typically develops after age 50, although it can begin earlier, and women are up to twice as likely to develop the condition. While age and sex cannot be modified, knee OA is strongly associated with lifestyle factors that can be controlled.
Modifiable risk factors driving knee OA development include:
To be effective, your knee OA treatment protocol should include weight management, dietary modifications, lifestyle interventions, knee stabilizer strengthening, and pain management strategies that do not involve drugs or steroids.
The role of fascia in human movement has only recently claimed the spotlight in musculoskeletal research, and its significance is still not fully understood. What we do know is that fascia plays a key role in biotensegrity – a state of constant elastic tension that holds the body’s structures in place during movement.
Fascia helps to guide and control movement, and transmits forces from one body segment to the next. It’s high haloranon content makes it slippery, reducing friction between various structures, and allowing nerves and blood vessels to glide smoothly.
Fascia is highly embedded with proprioceptors, making it a major pain generator.
Until recently, fascia was largely ignored in knee OA research, but new discoveries in the 2020s show that fascial structures play critical roles in knee pain, stiffness, biomechanics, and knee OA progression. The relationship between fascia and knee OA is a 2-way street – knee OA impacts fascia, making it denser and more fibrous, and reducing its gliding properties, while fascial restrictions can impact knee mechanics.
Fascial structures impacted by knee OA include:
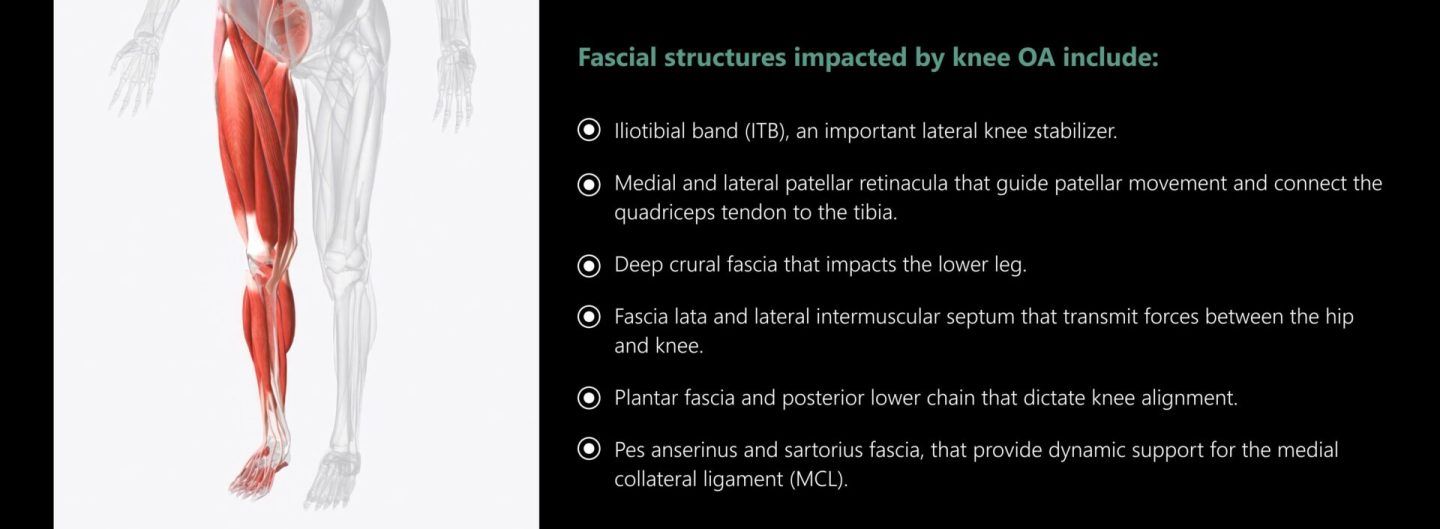
Treatment approaches like dry needling and fascial manipulation techniques can help to restore the functional properties of fascia, alleviating pain and improving knee stability and function. Fascial treatment is an integral part of a holistic approach to treating and resolving knee OA.
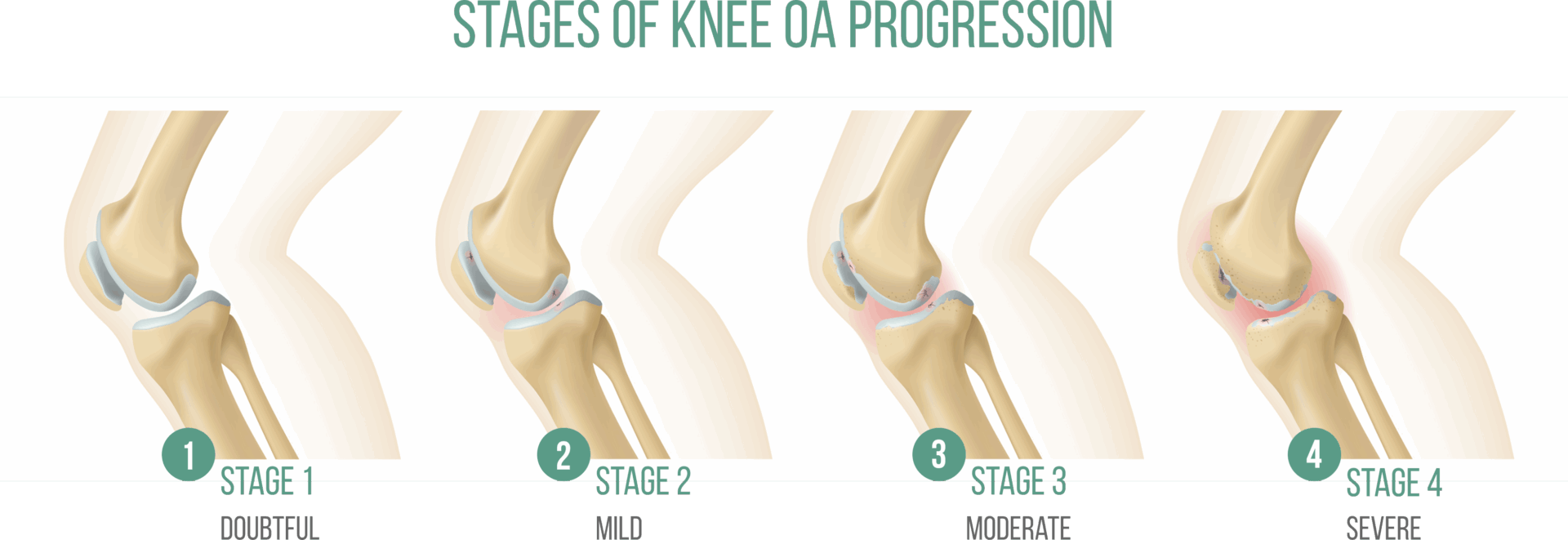
Unless treated in its early stages, knee OA becomes a progressive disorder that leads to severe degeneration of the knee joint over time.
Stages of knee OA progression include:
For decades MRI has been the gold standard for knee OA imaging, but in the 2020s, high resolution ultrasonography is rapidly gaining traction as the imaging modality of choice for a broad spectrum of musculoskeletal disorders. In addition to its clinical implications, many practical factors make ultrasound imaging a preferred choice for patients.

Practical advantages of ultrasound vs MRI:
When it comes to clinical aspects of knee OA assessment, MRI and ultrasound each has its distinct advantages, as shown in the following table:
| Feature | MRI | High-Resolution Ultrasound | Which is Better/Easier? |
|---|---|---|---|
| Sees cartilage clearly | Yes – best view | Only sees the surface (not thickness) | MRI |
| Sees bone marrow edema | Yes – very clear | No – can’t see inside bone | MRI |
| Detects inflammation (synovitis) | Good (best with contrast) | Excellent + shows blood flow | Ultrasound |
| Sees osteophytes (bone spurs) | Good | Very good (often sees them earlier) | Tie |
| Sees meniscus tears | Best | Only sees big or outer tears | MRI |
| Sees ligaments (ACL, etc.) | Best | Limited (only surface ligaments) | MRI |
| Cost | Expensive ($800–$2500+) | Inexpensive ($150–$450) | Ultrasound |
| Time in clinic | 30–60 minutes | 10–20 minutes | Ultrasound |
| Can be done in doctor’s office | No | Yes – right at bedside | Ultrasound |
| Guides injections | Rarely | Yes – live, very accurate | Ultrasound |
| Patient comfort | Loud, lying still in tube | Quick, no tunnel, can move knee | Ultrasound |
| Any risks / limits | Can’t do with pacemaker, claustrophobia | Almost none | Ultrasound |
Conventional treatment for knee OA centers on pain management, typically with topical and oral non-steroidal anti-inflammatory drugs (NSAIDs). Low dose opioids may be recommended for short-term use. Injections of glucocorticoids – steroid hormones with anti-inflammatory and immunosuppressive effects – may provide short-term relief for flareups. A cane, walker or braces can help reduce load on the knee while walking.
It is important to note that drugs like NSAIDs and steroids can have long-term detrimental effects on knee OA, accelerating degeneration. NSAIDs also have harmful effects on the liver, kidneys, GI tract and cardiovascular system, while steroids can affect blood sugar levels and cause weight gain, exacerbating metabolic issues that contribute to knee OA.
Holistic approaches to knee OA go beyond symptoms management, with the goal of improving mobility, stability and function. Treatment is not limited to the knee joint itself, but takes into consideration other factors such as densified fascia, weakened knee stabilizers, lifestyle factors and patient education.
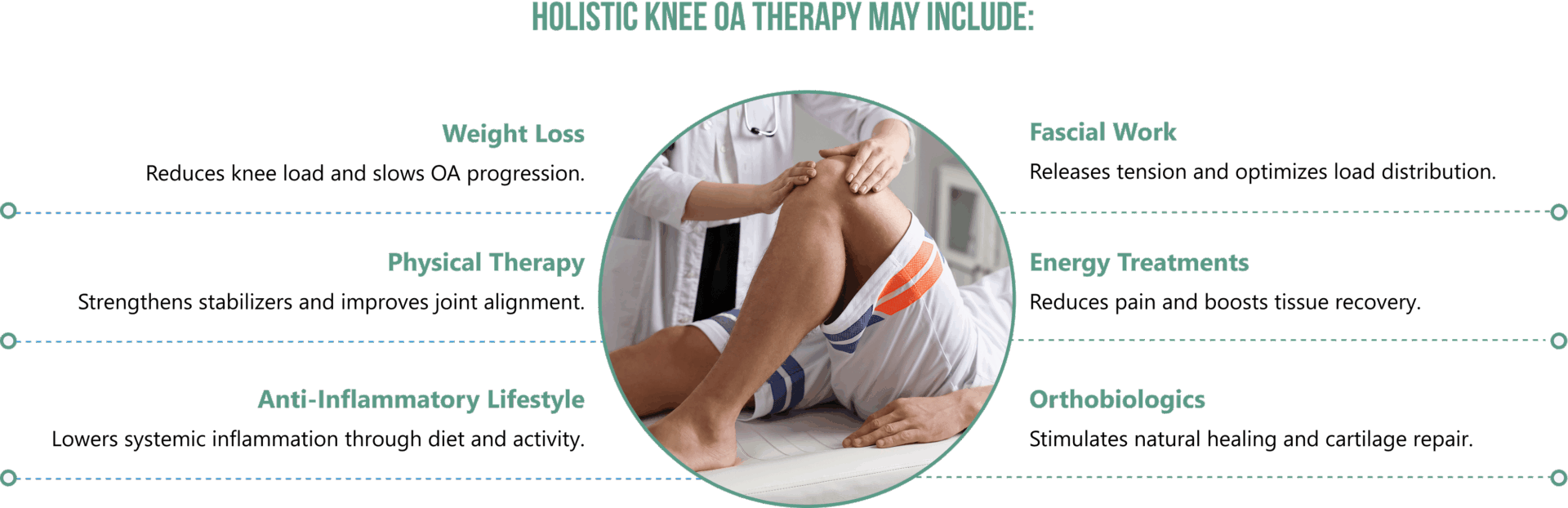
Holistic knee OA therapy may include:
Advancements in technology and research are having a profound impact on rehabilitative medicine, giving us powerful new tools for reducing pain and inflammation, healing damaged tissues, and even regenerating cartilage in osteoarthritic joints.
Extracorporeal shockwave therapy (ESWT) is a noninvasive treatment that uses high-energy acoustic waves to induce biological and physiological effects. ESWT reduces pain and inflammation, helps to realign and repair collagen fibers, promotes rehydration of synovial fluid and fascial tissues, and restores friction-free knee mechanics. ESWT is most effective when guided by high-resolution ultrasound imaging.
A recent study set out to compare the effectiveness of focal shockwaves (f-ESWT) and radial shockwaves (r-ESWT) on knee osteoarthritis. The study included 42 patients with bilateral knee osteoarthritis who were randomly assigned to receive 3 sessions of either f-ESWT or r-ESWT at 1-week intervals. Evaluation at 4 and 8 weeks found that both groups reported reduced pain intensity, improved knee range of motion, and improved walking mobility, with the fESWT group showing greater improvement.
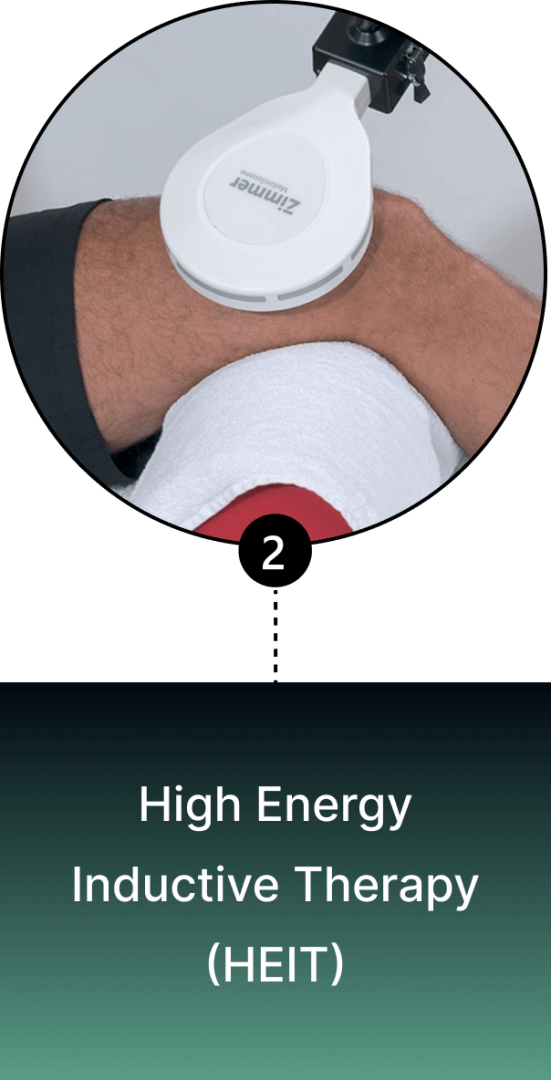
HEIT is a non-invasive technology that generates high-intensity electromagnetic fields to stimulate neuroplasticity. This FDA-approved methodology penetrates tissues, organs, and bones, to reactivate electrochemical function, regenerate nerve fibers, and enhance motor control.

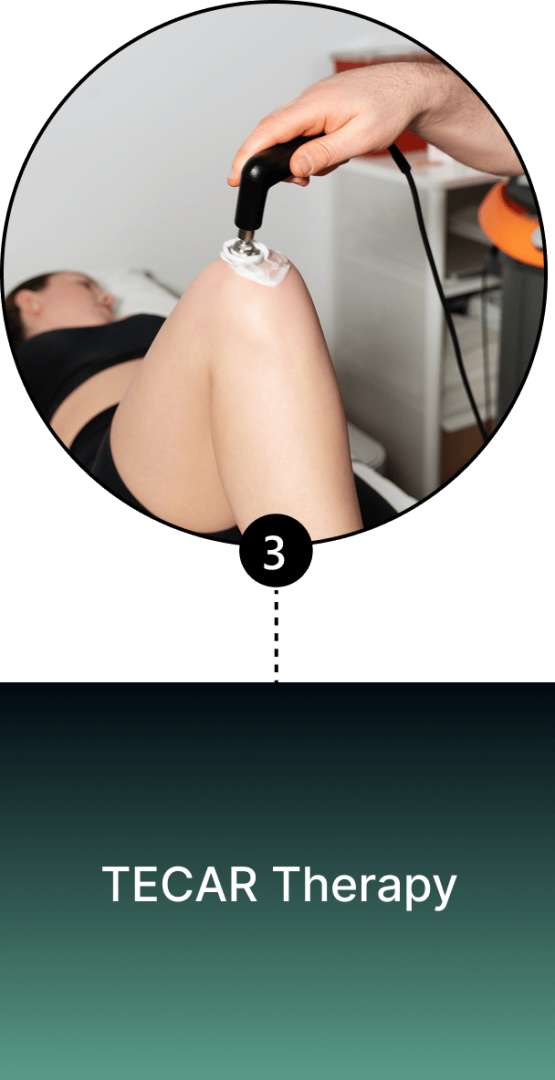

TECAR, an acronym for Transfer of Energy Capacitive and Resistive, is a non-invasive therapy that uses high-frequency electrical currents to deliver radiofrequency energy via a hand-held device, creating an electromagnetic field. TECAR triggers biological responses, including enhanced blood flow and oxygenation, increased cellular metabolism, improved lymphatic drainage, reduced inflammation, and pain relief.
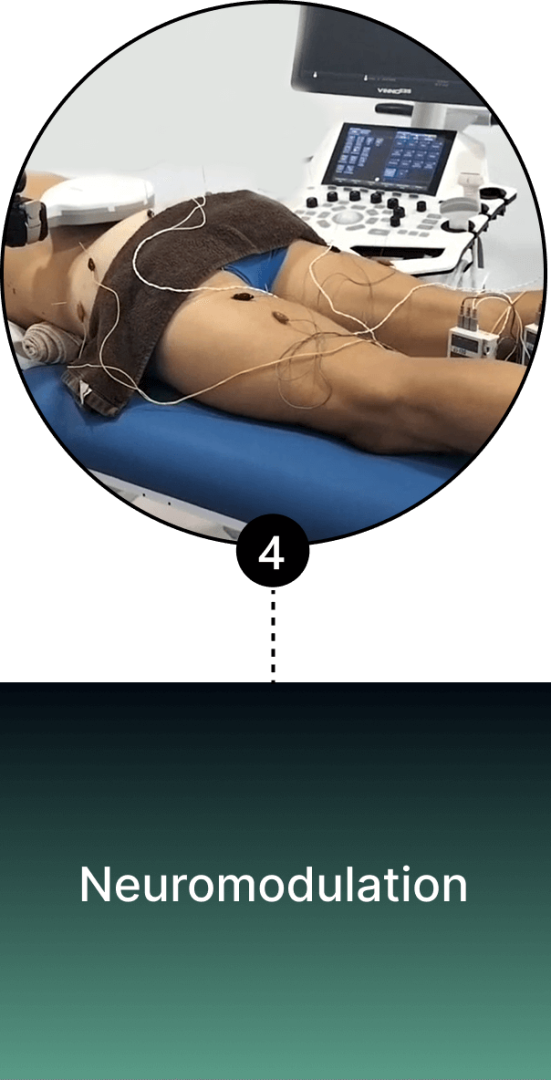
Neuromodulation
This non-invasive therapy uses electrical impulses to regulate or normalize nervous system function. It reduces pain and calms hypersensitized nerves that characterize knee OA. At the same time, it stimulates the surrounding muscles that support the knee, to enhance knee stability.
High intensity laser therapy harnesses targeted light energy via the processes of photomodulation and thermomodulation to stimulate healing in damaged tissues. One study divided 93 patients aged 50+ with confirmed knee OA into 3 groups: one group was treated with conventional physical therapy, another with exercise therapy, and a third with high-intensity laser therapy.
After 12 treatment sessions, patients were assessed for pain intensity, knee flexion range of motion, a timed up-and-go test, a 6-min walk test, and knee functionality compared to pre-treatment baseline measurements. Assessments were performed immediately after treatment and after 12 weeks. Results showed HILT to be significantly more effective across all metrics than physical therapy or exercise therapy.
PRP therapy injects a high concentration of platelets extracted from the patient’s own blood into the knee joint, triggering the release of biologically active agents such as growth factors, cytokines, lysosomes and adhesion proteins to initiate and accelerate tissue healing. There is strong evidence that high-platelet PRP therapy is effective for reducing pain and improving mobility in knee OA patients.

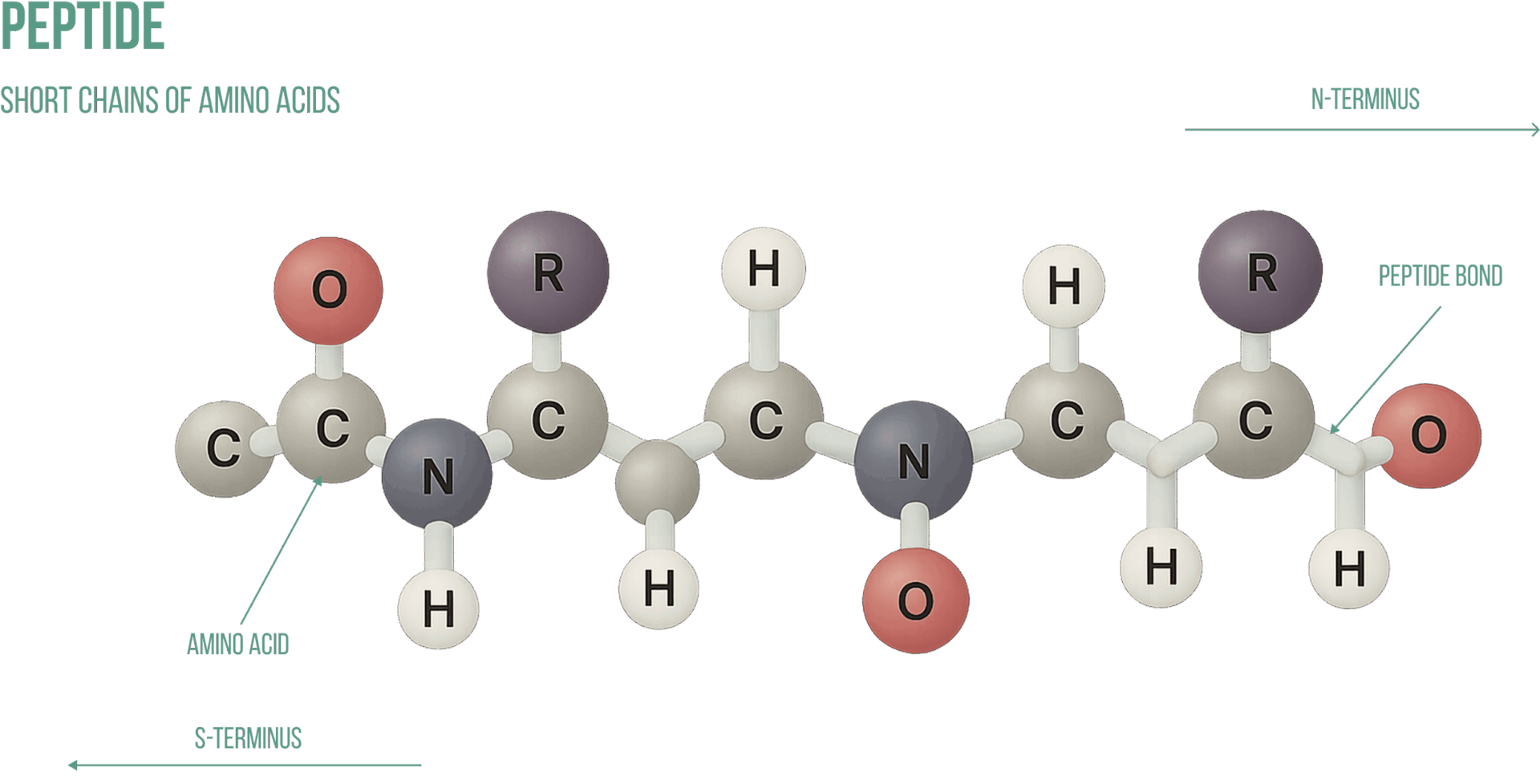
Peptides are short chains of amino acids that form the building blocks of proteins. Your body naturally makes its own peptides from dietary sources, but when specific peptides are injected into osteoarthritic joints in high concentrations, they have a regenerative effect. The use of peptides in knee OA is still in its exploratory stages, but so far they are receiving enthusiastic feedback from the regenerative medicine community.
In a recent study, 54 patients with knee OA were randomly assigned to three treatment groups and their knees were injected with either PRP, Hyaluronic Acid, or a peptide solution. While all patients reported improvements in pain and function, the peptide group reported the lowest pain scores 3 months post-treatment.
While several peptides hold promise as adjuncts to knee OA treatment, BPC-157 is recognized as the single most effective peptide for knee OA pain and function. Administered in cycles of 3-6 daily injections, patients treated with BPC-157 report up to 90 % pain reduction lasting months to years after a single cycle. Peptide injections should be done by a qualified clinician under ultrasound guidance to avoid cartilage damage.
Exosomes are nano-sized extracellular vesicles derived from various cells. Exosomes act as messengers that deliver proteins, miRNAs, and lipids to modulate inflammation, promote cartilage regeneration, and reduce subchondral bone loss. When injected into osteoarthritic joints, exosomes are shown to regenerate cartilage, reduce synovitis, and promote bone remodeling.
Common sources of exosomes include:
The following chart shows the efficacy of various exosomes for pain reduction and cartilage regeneration:
| Exosome Source | Cartilage Repair (Preclinical Score Improvement) | Pain Reduction (Clinical %) | Key Trial/Study |
|---|---|---|---|
| hUC-MSC | 40–60% | 40–50% | 2025 J Transl Med (n=20) |
| BM-MSC | 30–50% | 30–40% | Meta-analysis (rat models) |
| PRP | 20–40% | 25–35% | 2025 Int J Mol Med |
| iPSC-MSC | 50–70% (projected) | TBD (Phase 3 ongoing) | Cynata CYP-004 |
BMAC (Bone Marrow Aspirate Concentrate) and MFAT (Micro-Fragmented Adipose Tissue) are orthobiologics rich in mesenchymal stem cells (MSCs), growth factors, and anti-inflammatory mediators. When injected into osteoarthritic joints, they are shown to modulate inflammation, promote cartilage repair, and delay OA progression. BMAC is harvested from iliac crest bone marrow, while MFAT is derived from adipose tissue from the thigh or abdomen.
BMAC is a more concentrated source of stem cells and growth factors than PRP and can be more regenerative for advanced knee OA. Both BMAC and MFAT deliver similar results, although BMAC is generally used for younger, bone-involved OA, while MFAT is considered a better fit for elderly patients and those with higher body weight. MFAT is often combined with PRP or BMAC to maximize the benefits of all three therapies.
Alpha 2 macroglobulin (A2M) is a naturally occurring blood plasma protein that acts as a carrier for numerous proteins and growth factors. As a protease inhibitor, A2M reduces inflammation in arthritic joints and helps to deactivate a variety of proteinases that typically degrade joint cartilage. When concentrated A2M is injected into osteoarthritic joints, it halts the progression of the disease and initiates cartilage repair and regeneration.
Hyaluronic acid is a natural component of joint synovial fluid. Its slippery gel-like properties provide lubrication that reduces friction, enabling joints, muscles and fascia to move freely without pain. In knee OA patients, synovial hyaluronic acid tends to break down, causing bony structures to rub against one another. Hyaluronic acid replenishes synovial fluid to reduce friction and relieve pain.
Prolotherapy injects a neutral dextrose solution into knee tissues, initiating a local inflammatory response that triggers a healing cascade. Research indicates that Prolotherapy may play a role in chondrogenesis – the regrowth of cartilage. Prolotherapy has been shown to reduce pain and stiffness, and improve knee function and quality of life in knee OA patients.
Nerve hydrodissection is a minimally invasive procedure aimed at relieving osteoarthritic knee pain. It targets the genicular nerves that transmit pain signals from the knee joint. The technique involves ultrasound-guided injection of a solution made up of saline, dextrose or PRP, to separate the nerve from surrounding tissues and relieve nerve compression.
Dry needling targets myofascial trigger points – tiny nodules of tightly contracted fibers that cause pain and interfere with muscle action. Trigger points can contribute to knee OA pain by disrupting the action of knee stabilizers. The dry needling procedure inserts filament-thin, non-medicated (dry) needles into active trigger points, triggering a twitch response that relaxes taut fibers and immediately relieves pain.
The Stecco method is a specific, evidence-based technique that targets densified and dysfunctional fascia, to release entrapped nerves and blood vessels, and restore fascia’s elastic and gliding properties.


Joint osteoarthritis is primarily a lifestyle-induced disease linked to obesity, systemic inflammation and metabolic disorders. Knee OA can be prevented, but it requires modification of multiple behavioral factors, to prevent knee degeneration and dramatically improve overall health.
Request a gait analysis and gait retraining, to correct inefficient gait mechanics that contribute to knee OA.

There are many new and exciting options that dramatically improve knee OA treatment outcomes, but they are rarely found under one roof, and many clinicians lack the training and expertise to effectively use them. The clinic at NYDNRehab features a broad range of regenerative technologies and advanced therapies to effectively treat knee OA. Dr. Kalika’s experience and expertise in diagnosing and treating musculoskeletal conditions is unrivaled, making NYDNRehab the clinic of choice for knee OA in NYC.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































