Our patient is a female in her 20s who came to us with severe right-sided neck pain, consequent to a dry needling session at another clinic. Her pain spanned from the upper trapezius area and down the medial scapular border. The patient has a history of chronic right-sided neck pain and previously had a cervical discectomy – a procedure where the disc is removed and the bones fused together – but the surgery provided no relief.
The patient had been to multiple therapists, chiropractors and medical doctors whose treatments made her symptoms worse. Diagnostic imaging modalities revealed nothing abnormal, and no one was able to help her. She was told by one doctor that she had shoulder labral tears, but nothing was done to address the condition. She came to NYDNRehab in hopes that we could find a solution for her chronic pain.
During the clinical exam, we assessed the patient to have:
The patient’s scapular instability was a mixed type, with right scapular dyskinesis and bilateral protracted scapular position. She exhibited hypermobility, with a negative Beighton score for EDS syndrome. Both shoulder joints tested positive for instability. However both of her shoulder joints tested positive to instability testing.
Results of a neurological exam were normal, and palpation of the cervical spine did not elicit pain. However, palpation of the left upper trapezius elicited pain and tenderness. We also found multiple fascial densifications along the retro-lateral line.
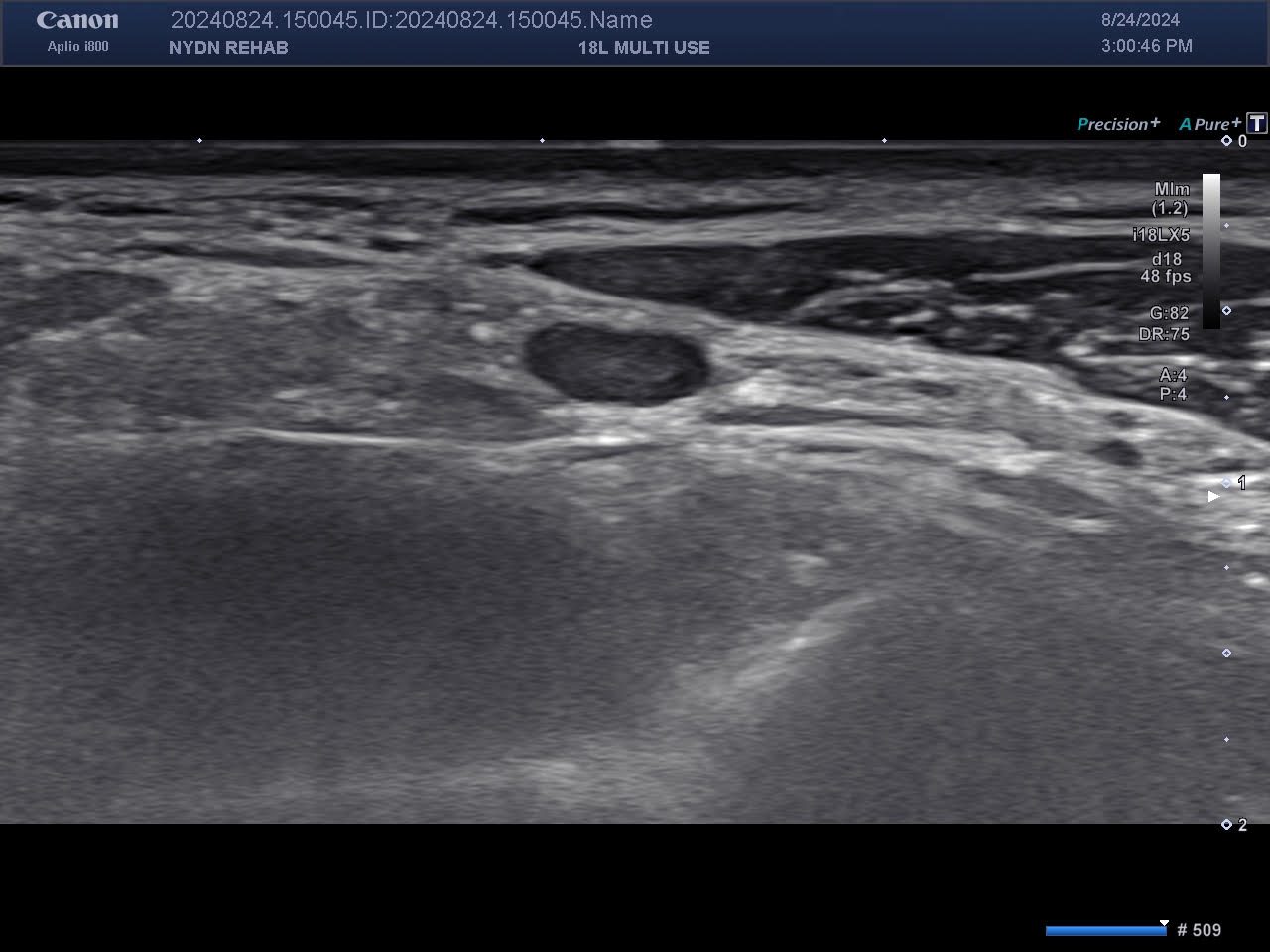
When visualized with ultrasound imaging, both rotator cuffs appeared normal, but dynamic testing found the right posterior labrum to be hypermobile. We found an enlarged singular lymph node adjacent to the spinal accessory nerve in the fascial plane between the sternocleidomastoid muscle and the upper trapezius. Pressure on the enlarged lymph node reproduced her symptoms.
When asked if she had been sick during her dry needling procedure, the patient replied that she had been diagnosed with a COVID infection the following day. We deduced that the dry needling procedure had induced further inflammation of the lymph node, which was already swollen due to Covid. This in turn irritated the spinal accessory nerve, causing referred pain that precisely replicated the patient’s symptoms.
Dry needling is a procedure intended to target myofascial trigger points. However, without the advantage of ultrasound imaging, dry needling performed “blind” can do more harm than good, with the needles penetrating nerves, blood vessels and other structures. Ultrasound not only confirms the presence of trigger points, but it is an invaluable tool for guiding needling procedures, to precisely hit the targeted tissues without harming other structures.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















