Our patient is a 52 year-old female runner who came to us after unsuccessful treatment elsewhere, complaining of mild low back pain shooting down her right leg. She explained that she had never had low back pain before, and that her locus of pain was slightly lower than her lumbar spine and closer to her right gluteal muscle. Her goal was to return to pain-free running.
A previous doctor had referred her for MRI, which revealed a bulging disc at L4-L5. Two epidural steroid injections (ESIs) did not resolve her back and leg pain. She was referred to physical therapy, where she was prescribed a regimen of planks and other core strengthening exercises, along with stretching. After four months of therapy, she was still in pain.
The patient had no tenderness over her lumbar spine, and exhibited no instability in her walking gait. A stress test of her lumbar spine found no instability or abnormal motion.
Further examination revealed:
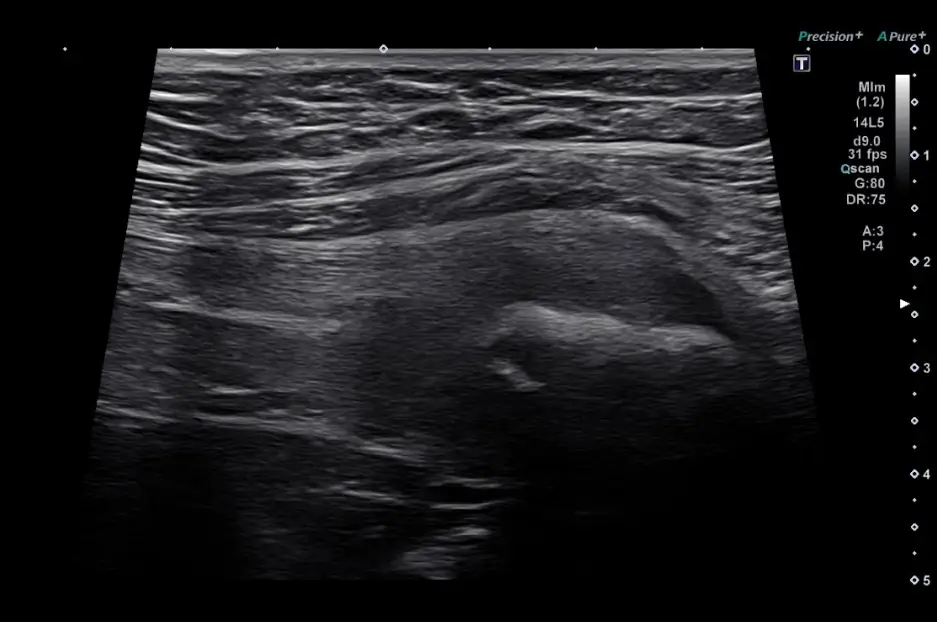
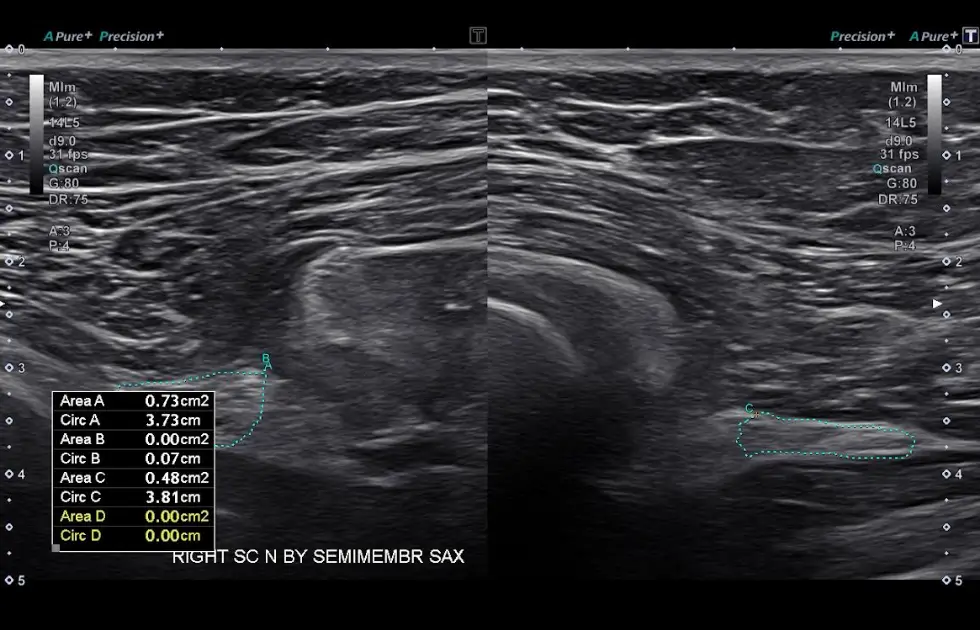
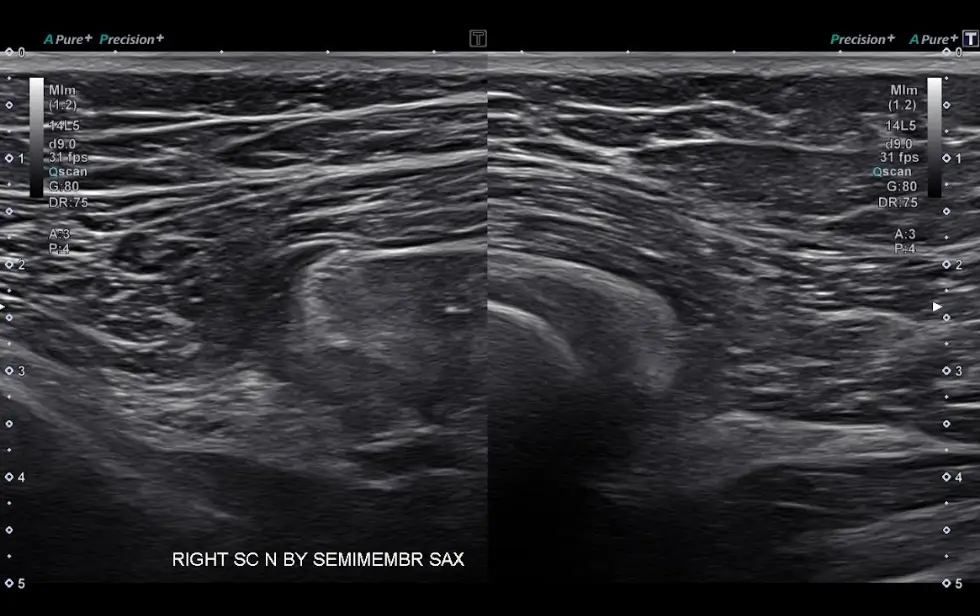
High-resolution ultrasound revealed:

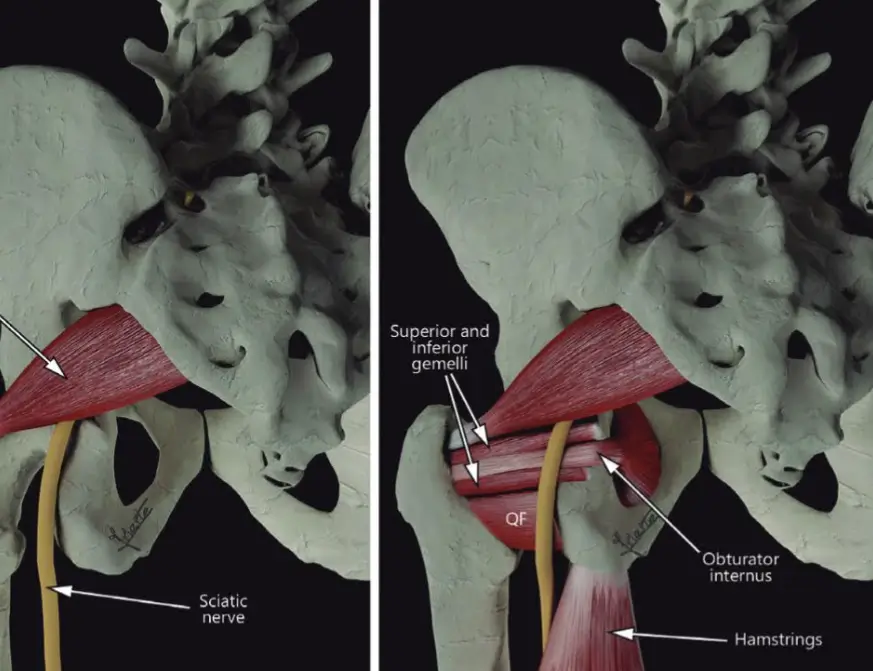
We concluded that the patient had dysfunction and instability in the right SIJ, along with hamstring syndrome – proximal hamstring tendinopathy that affects the sciatic nerve, causing symptoms of pain down the right leg that mimic spinal nerve root compression.
We used focused shockwave therapy with ultrasound guidance to precisely target the semimembranosus tendon, to encourage collagen fiber realignment. The patient wore a special belt to support her SIJ during physical therapy to address her SIJ instability. She also did isometric hamstring exercises to treat her hamstring tendinopathy.
At eight weeks, we conducted ultrasound-guided dry needling to eliminate trigger points, and hydrodissection to release the sciatic nerve and restore gliding. At this point, 90% of her symptoms had been eliminated.
We then performed a 3D running gait analysis and discovered she was over-striding, which no doubt contributed to her pain and dysfunction. After gait retraining the patient was able to resume her running schedule of up to 40 miles a week. We provided her with an in-depth exercise program to improve her pelvic strength and stability.
Diagnosis based on symptoms alone can lead to inappropriate and ineffective treatment that prolongs the patient’s pain. MRI alone is not adequate to uncover the underlying cause of pain. Compared to ultrasound, MRI has fairly low resolution, and renders only static images of the body’s structures.
Ultrasound lets us visualize long structures like nerves, muscles and fascia along their entire paths, in real time. It gives us images of fascial aponeurotic extensions, loss of fascial gliding, fascial densifications, muscle fatty infiltration, and trigger points. With ultrasound, we can also dynamically test the sacroiliac joint ligaments and cluneal nerves, none of which is possible with MRI.
Only imaging with dynamic high-resolution ultrasound can give us a complete picture of the structures as they interact. High-resolution diagnostic ultrasound lets us accurately identify the true source of our patients’ pain and dysfunction, helping to ensure fast and effective treatment.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















