Our patient is a tall, slender 36 year-old female complaining of joint pain throughout her body, with her right (dominant) elbow causing the worst pain, and significantly interfering with her job and recreational activities. She also reported bloating, sluggish bowel movements and constipation. She had seen a number of doctors, including orthopedic surgeons, physical therapists, and pain management physicians, and had numerous x-rays and MRIs, but they were unable to ascertain the cause of her pain or alleviate it.
The patient’s rheumatology reports were normal, and there was no history of major trauma, although she reported a history of multiple sprains, strains and subluxations during physical activities. Previous tests revealed absence of orthostatic hypotension or dysautonomia, cardiovascular or respiratory disease, urinary or gynecological symptoms, or hormonal imbalance.
A postural assessment revealed layered postural syndrome, marked by weak abdominal and gluteal muscles, tight hip flexors, rounded upper spine and tight pectoral muscles. Her knees were hyperextended when standing, and she had difficulty maintaining balance in a single-leg stance. Her appearance was typical of joint hypermobility or Ehlers Danlos syndrome.
Her Beighton score – a test for joint hypermobility – was five out of nine. She exhibited a large carrying angle at the elbow of her dominant arm. An examination of her medial and lateral elbow showed moderate hypermobility with mild tenderness upon palpation. Palpation of the supinator muscle caused significant pain.
Ultrasound imaging showed a normal appearance of the muscles and tendons attached to the medial and lateral epicondyle, and normal appearance of the distal biceps and triceps tendons. All elbow joints appeared normal, as did the ulnar nerve.
The median nerve appeared normal except for a thinning at the bottom of the flexor arcade, especially during resistive pronation. Palpation of the flexor digitorum superficialis (FDS) reproduced her medial elbow pain.
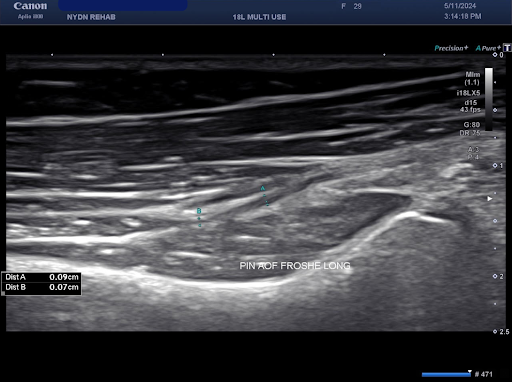
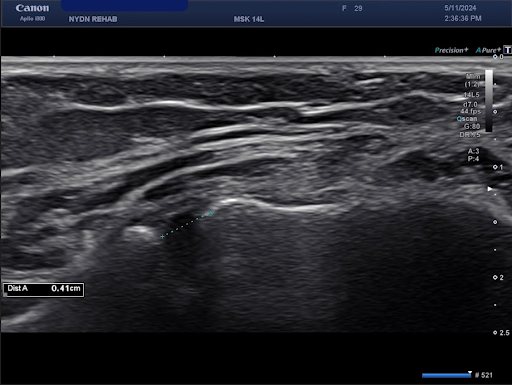
The radial nerve in her distal arm appeared normal until the nerve split into its sensory and motor branches. The motor branch where the radial nerve entered the arcade of Frohse felt tender, and palpation produced symptoms similar to lateral epicondyle pain.
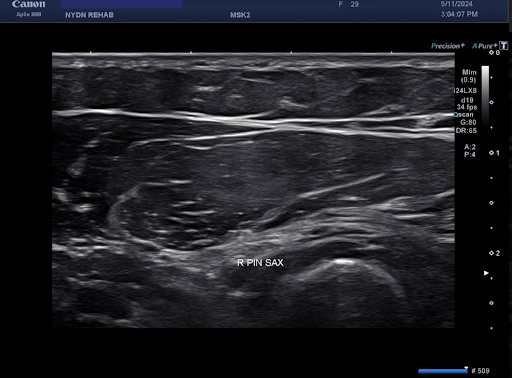
There was a thickening of the posterior interosseous nerve just proximal to the arcade of Frohse, and the fascia between the supinator and the extensor carpi radialis brevis appeared abnormal.
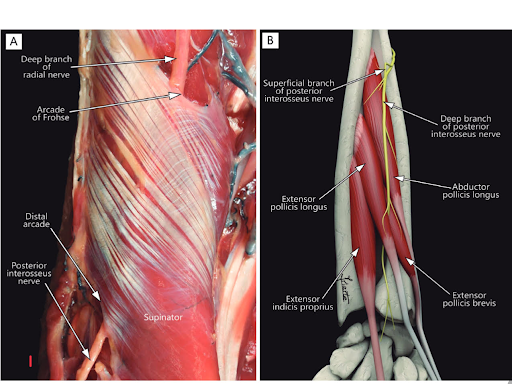
We determined that the patient had general joint hypermobility syndrome, with posterior interosseous nerve compression in the arcade of Frohse and median nerve compression at the flexor arcade.
Joint hypermobility syndrome (JHS) and Ehlers Danlos syndrome (DHS) are not particularly rare, but most doctors are not familiar enough with the condition and are not equipped to diagnose it or describe the cardinal signs that produce symptoms, such as:
It isn’t always possible to distinguish between mild EDS and JHS, but the treatment is essentially the same, and treatment should be based on clinical and radiological findings.
Familiarity and experience with patients who suffer from JHS and EDS is required to accurately diagnose and treat patients presenting with such symptoms. Only a hypermobility-specific exam using high resolution diagnostic ultrasonography can provide adequate information for diagnosis and treatment of patients within the JHS-EDS spectrum.
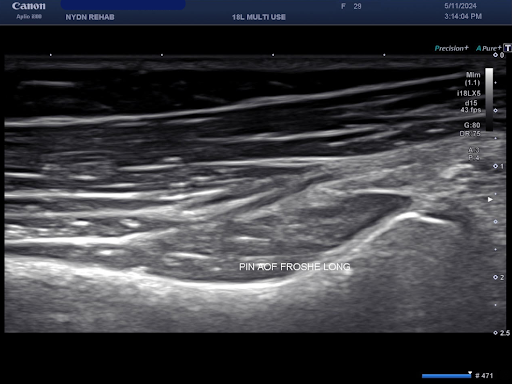
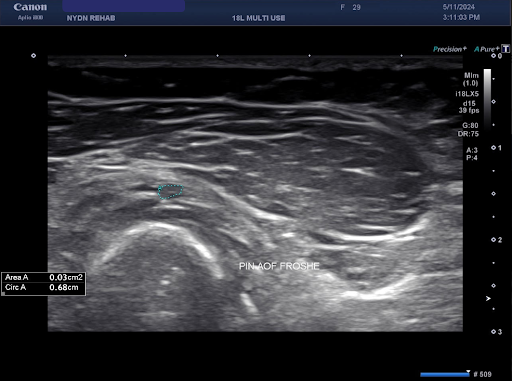
Notch sign of PIN in Arcade of Frohse in the long axis, without and with calipers
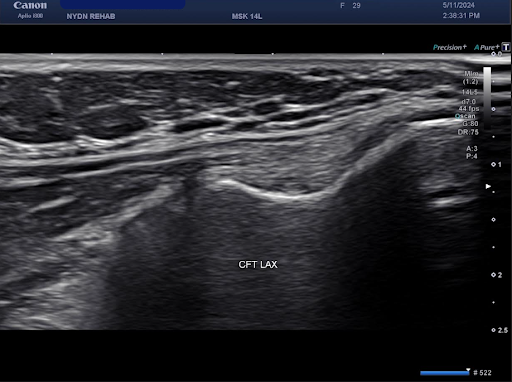
Dynamic testing of medial elbow hypermobility


Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















