Our patient is a 19 year-old male suffering from 3 years of sternal and lower frontal rib cage pain. The patient was a bodybuilder whose weight training regimen included chest presses, pushups, dips and other exercises that recruited muscles in the pectoral region. Various attempts to treat him had been unsuccessful, and his pain eventually prevented him from doing any exercise. He came to our clinic all the way from Indiana looking for help.
The patient had previously received a diagnosis of costochondritis – inflammation of the rib cage cartilage. However, over the course of 30 years seeing patients with rib cage pain, I have concluded that 95+ percent of rib cage pain is incorrectly dismissed as costochondritis, which in my opinion is an outdated medical diagnosis that does not exist. The suffix “itis” implies inflammation. However, cartilage tissue is largely avascular and rarely inflamed, and there is zero scientific evidence to support the existence of costochondritis.
A physical exam revealed that the patient’s pain was more pronounced when he rotated his torso. He was able to reproduce more severe pain when he stretched his arms forward and rounded his thoracic spine.
Palpation revealed sensitivity at the second rib head where it connected to the manubrium of the sternum. There was also sensitivity along the ante-lateral fascial line, with multiple fascial densifications along the lower ribs that restricted chest expansion while breathing and limited trunk rotation. There was also a load transfer failure in ribs 5-6-7, with a shift to the right side.
Ultrasound imaging revealed the following:
Image 1: Decreased intercostal space between ribs 5-6-7 (intercostal muscles appear white).
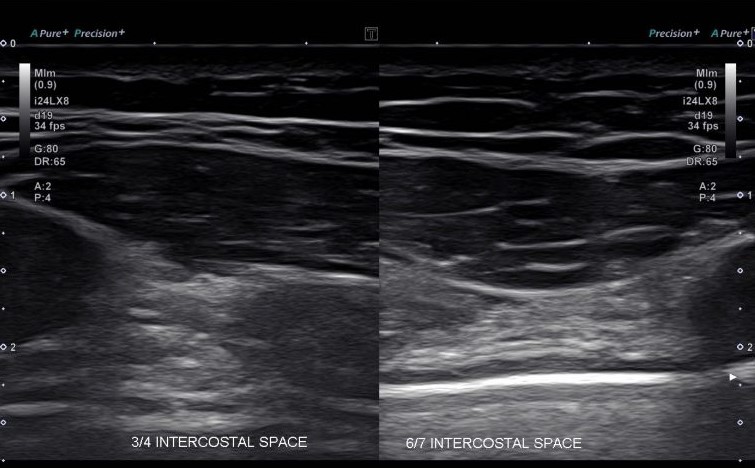
Image 2: Normal intercostal space between 2-3-4.
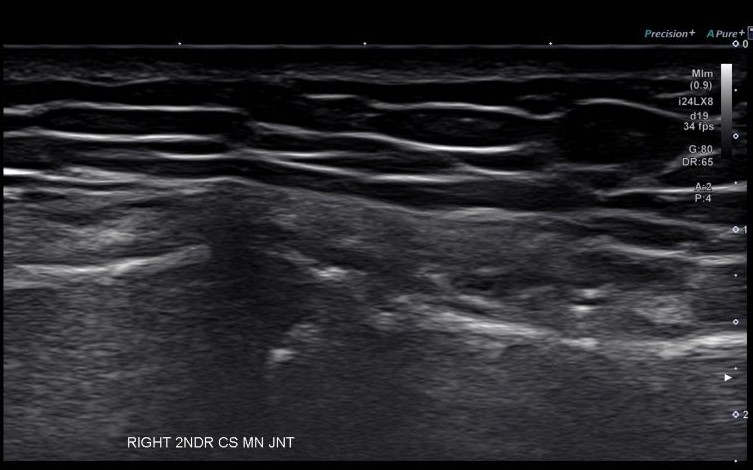
We began with fascia manipulation therapy to restore the integrity of densified fascia along the lower ribs, which provided significant improvement after a single session. We used shockwave therapy to treat tissues at the 2nd rib manubrium joint, and used the thoracic ring approach to correct rib cage muscle activation patterns. We sent our patient home to Indiana in a much-improved state, with instructions for home exercises and maintenance.
It is not uncommon for medical doctors to dismiss undiagnosed musculoskeletal pain as some generic condition without substantial evidence. From a holistic perspective, we know that most musculoskeletal issues are multifaceted and require an integrative approach. Intense physical activities like weight lifting that overload soft tissues can cause fascia densifications that restrict movement and cause pain. Static and dynamic stretching after intense exercise can help protect fascia from becoming densified over time.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















