Our 14 year-old female patient arrived at our clinic with her mother, complaining of mild left shoulder pain. The patient was physically active and athletic. She was currently playing golf on a regular basis and desired to return to playing tennis.
A previous doctor had diagnosed her condition as subacromial impingement and referred her for physical therapy, which she had done over the summer, with little improvement in her shoulder pain. The patient and her mother were not overly concerned, and believed the original diagnosis to be correct.
Our clinical exam revealed several factors:
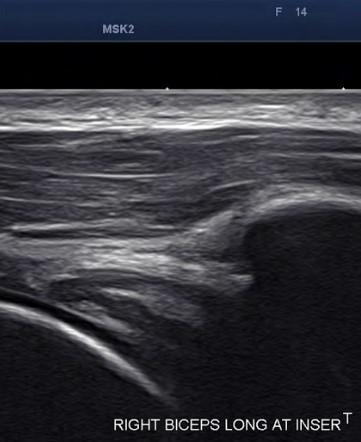
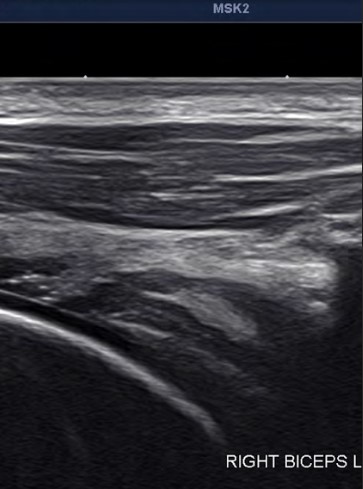
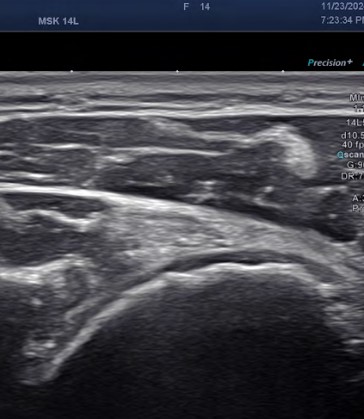
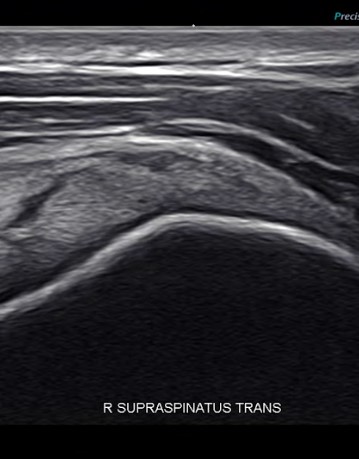
High-resolution diagnostic ultrasonography alerted us to several issues:
We referred the patient for an MRI to confirm our findings from the ultrasound exam. We recommended that she abstain from all physical activities, including golf, until further treatment.
The MRI results confirmed the presence of rotator cuff lesions.

We used ShowMotion technology to evaluate the patient’s shoulder movement parameters. ShowMotion is an objective tool for analyzing joint movement quality with the use of wearable motion tracking sensors. We asked the patient to perform a series of joint-specific movements, and confirmed a secondary dyskinesia due to her rotator cuff lesions and shoulder instability. This was complicated by joint hypermobility.
Showmotion is the first technology of its kind to show the kinematics of the glenohumeral joint and the scapula, and their relationship during shoulder girdle movement. It is an indispensable tool for precise rehabilitation of shoulder disorders.
We used shockwave therapy and PRP injections to reduce pain and inflammation and stimulate healing of the rotator cuff lesions.
We used the Neuralign Shoulder Pacemaker, a shoulder rehabilitation device that interacts dynamically with the patient during rehabilitation to stimulate efficient muscle recruitment patterns, enhance movement quality, and restore optimal muscle balance.
The patient showed substantial improvement after 3 months of treatment, and was able to return to golf and tennis after 6 months.
Shoulder impingement is always an outcome of other mechanisms of shoulder injury, and never the cause itself. In any rotator cuff tendinopathy or a-traumatic tear – a continuation of tendinopathy – we must first establish the cause and mechanisms of injury. Failure to do so will lead to ineffective treatment and eventual progression to more tears and surgery. The clinical exam alone is not enough to diagnose subacromial impingement – it must be confirmed with diagnostic imaging.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















