
Achilles Tendinopathy
Personalized boutique services supported by cutting-edge
integrative diagnostics and advanced holistic therapies.
Dr. Kalika and Dr. Brosgol are Experts
in Achilles Injury Rehab
Clinical director & DC RMSK
Verified Expert Profiles
Dr. Lev Kalika, DC, clinical director of NYDNRehab, is an internationally recognized expert in diagnostic and musculoskeletal ultrasonography, with multiple research publications to his credit. Dr. Kalika has studied with some of the world’s most prestigious experts in diagnostic, fascia, and nerve ultrasonography, and has presented his research at multiple international conferences.
“My 20+ years of success in treating tendon injuries comes from a deep understanding of tendon pathologies, and from the ability to visualize each individual tendon. No two tendons are alike in their anatomy, biomechanics and function. Most tendons are superficial structures, and are much better visualized by high resolution ultrasonography versus MRI. A distinct advantage of diagnostic ultrasonography over MRI is its ability to visualize muscles and tendons in motion.” – Dr. Lev Kalika
Dr. Kalika is an active member of the American Institute of Ultrasound in Medicine (AIUM), and has developed his own unique approach to Dynamic Functional and Fascial Ultrasonography.

Dr. Yuri Brosgol, MD is a neurologist with 25+ years of experience in treating myofascial and chronic pain conditions. In addition to being a pioneer in orthobiologics and fascial release techniques, Dr. Brosgol is a functional medicine specialist, providing a holistic and nuanced approach to treating common sports injuries and chronic pain syndromes.
Together, Dr. Kalika and Dr. Brosgol are revolutionizing the way Achilles tendinopathy is diagnosed and treated. The clinic at NYDNRehab features some of the most advanced technologies and therapies available for rehabilitative medicine.
Achilles Tendon Architecture and Function
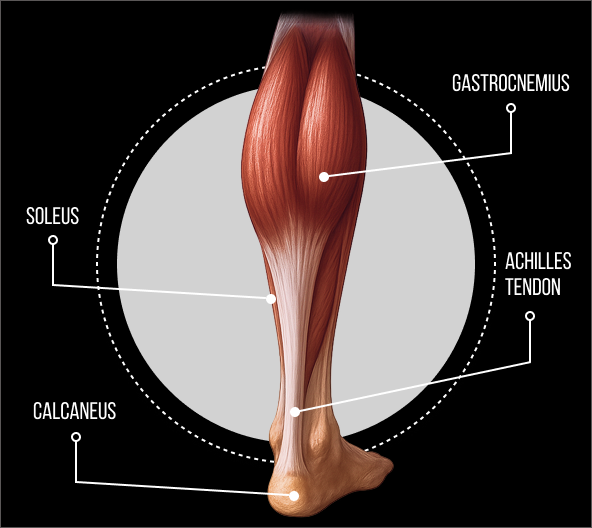
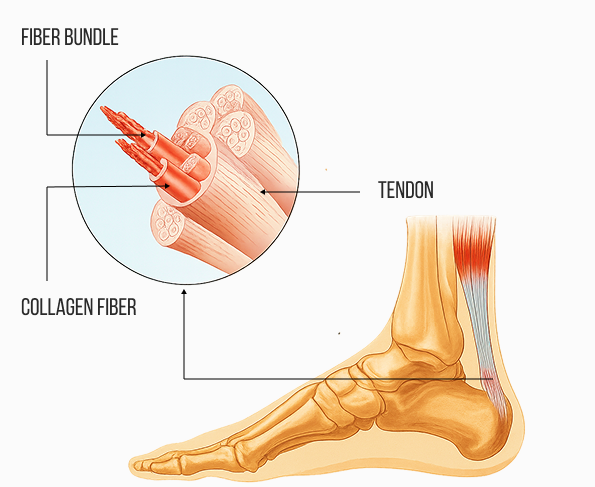
The Achilles tendon is foundational to ankle functionality, human locomotion, gait, and posture. It is formed at the convergence of the soleus muscle with the lateral and medial heads of the gastrocnemius – collectively called the triceps surae. These muscles work together to plantarflex the foot (point the toes downward) at the ankle, enabling forward and upward propulsion. Unlike the highly vascular tissue of the calf muscles, the Achilles tendon is a tough connective tissue made up of collagen, with limited vascularity.
The Achilles tendon plays a crucial role in proprioception – the body’s ability to sense its dynamic position relative to the ground. The Golgi tendon organ (GTO) is a key proprioceptor that provides feedback to the brain about changes in muscle length, tension, and joint position, affecting stability, balance and coordination. Injuries to the Achilles tendon can impair proprioceptive feedback, increasing the risk of further injury.
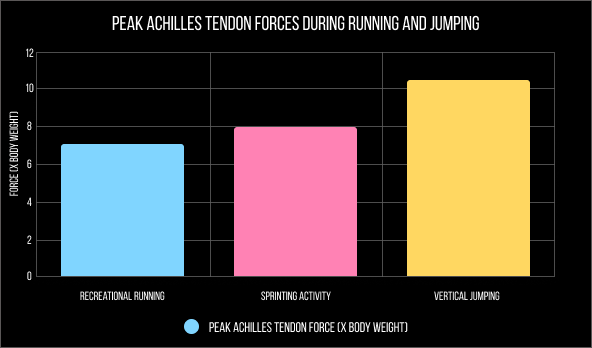
While extremely tough, the Achilles tendon is vulnerable to injury and rupture due to the immense forces acting on it during physical activity. The tendon is able to withstand forces as high as 7-10 times your body weight during high-impact activities like sprinting, running and jumping, but its limited blood supply makes it prone to repetitive overuse injuries. Low blood supply also makes the Achilles tendon slow to heal.
Achilles Tendinopathy Causes and
Risk Factors
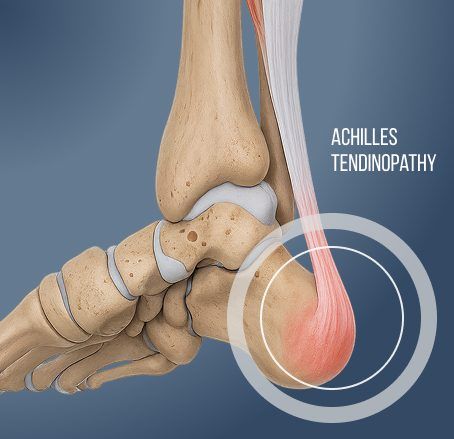
Achilles tendinopathy is a painful condition marked by swelling and impaired function of the Achilles tendon. Tendinopathy is typically caused by overuse, repetitive strain, or microtrauma, and is commonly seen in runners and athletes. There are two main subtypes of Achilles tendinopathy – insertional and noninsertional.
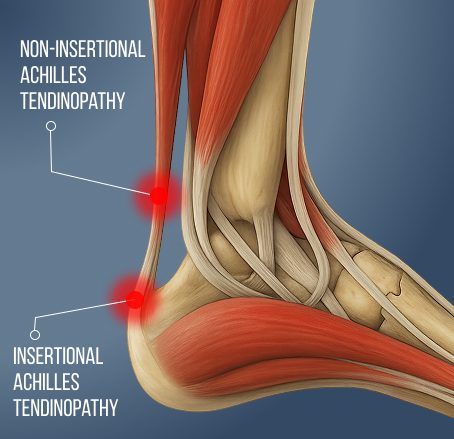
Insertional Achilles tendinopathy:
- Occurs where the Achilles tendon attaches to the heel bone (calcaneus).
- Involves degeneration or inflammation of the tendon at the insertion site.
- More challenging to treat due to poor blood supply at the insertion and mechanical stress from the bone.
- Symptoms include pain and stiffness at the back of the heel that worsens with activity, especially when running and climbing stairs.
- Caused by tight calf muscles, improper footwear, repetitive stress, and metabolic conditions like obesity and chronic inflammation.
Non-Insertional Achilles Tendinopathy:
- Affects the mid-portion of the Achilles tendon, typically 2–6 cm above the insertion point.
- Characterized by tendon degeneration due to microtears and collagen disorganization.
- No significant inflammation.
- May include tendon thickening and tender palpable nodules.
- Symptoms include pain and swelling in the mid-portion of the tendon, stiffness after a period of inactivity, and pain during and after activity.
- Caused by repetitive overuse, tight or weak calf muscles, poor training technique, or sudden increases in training intensity.
Causes and risk factors of Achilles tendinopathy differ in people under age 40 versus older adults. driven by differences in activity level, biomechanics, and tissue changes. In younger people, especially athletes, Achilles injuries are mostly due to repetitive stress from sports, high-intensity training, sudden increases in activity, or improper technique.
A 2025 study of 389 subjects aged 8-79 used ultrasound and sonoelastography to evaluate healthy Achilles tendon properties in terms of length, thickness, and viscosity, all three of which increase with age. The researchers surmised that age-related changes in Achilles tendon structure may limit its capacity to store and release energy in older adults. Achilles tendon injuries in older adults may require a different treatment approach than those used for younger people.
In older recreational athletes, Achilles ruptures are more frequent and degeneration-driven due to weaker, less resilient tendons. Research indicates that medications like statins, corticosteroids, and fluoroquinolone antibiotics increase the risk of tendon injuries. Metabolic disorders like obesity, chronic systemic inflammation and diabetes also increase tendon injury risk.
Precision Diagnostics Underscore
Successful Tendinopathy Treatment
To successfully treat Achilles tendinopathy, it is critical to visualize the tendon in motion, in real time. This can only be achieved with high-resolution ultrasonography. The clinic at NYDNRehab features the highest-resolution ultrasound currently available, with capabilities for sonoelastography and superb microvascular imaging (SMI). Dr. Kalika is a world-recognized expert in diagnostic ultrasonography.
Ultrasound lets us precisely identify the site and scope of injury, compare the injured and non-injured legs, detect pathological vascularization via SMI, and test for tendon stiffness via sonoelastography. Stiffer tendons are more capable of storing and releasing elastic energy – think of a thick versus thin rubber band being maximally stretched and released.
Healthy Achilles tendons are composed of well-organised, parallel collagen fibres with bright and dark hyperechoic bands. In people with Achilles tendinopathy, ultrasound lets us visualize areas of disorganized, unstructured, non-parallel collagen fibres, with thickened hypoechoic portions, indicating tendinosis – a chronic, degenerative condition of the tendon.
High-resolution ultrasound imaging also helps us estimate the involvement of the Kager’s fat pad – a mass of adipose tissue located posterior to the ankle joint complex. The Kager’s fat pad helps to protect the blood vessels that feed the Achilles tendon, and contributes to ankle stability and biomechanics. Recent research indicates that asymmetric positioning of the Kager’s fat pad relative to the Achilles tendon during maximum passive ankle dorsiflexion is strongly associated with Achilles tendinopathy.
High-resolution diagnostic ultrasonography empowers us to uncover all factors involved in Achilles tendon injuries, enabling us to customize treatment protocols based on the unique characteristics of each patient’s injury. Ultrasound also provides us with an objective tool for monitoring the healing process in response to treatment, ensuring that the patient has fully recovered before being released to physical activity.

Biotensegrity Governs Ankle Stability
and Biomechanics
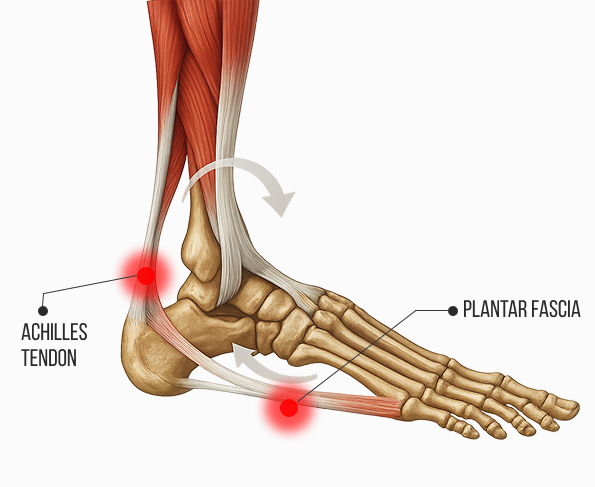
Mechanical action of the Achilles tendon is intimately related to the plantar fascia – the taught band of connective tissue that spans the bottom of the foot, attaching the calcaneus to the toes. Together, the triceps surae, Achilles tendon and plantar fascia form a mechanical complex due to their shared attachment to the calcaneus. They work in concert to absorb shock, stabilize the foot and ankle, and generate propulsive force during walking, running and jumping.
Both the Achilles tendon and the plantar fascia are made up of collagen fibers, but fascial tissue has a higher elastin content than tendons, making it more elastic, and fascia is infused with hyaluronic acid, giving it slippery properties that allow for gliding without friction. Like the Achilles tendon, the plantar fascia stores elastic energy as it stretches, and releases it as it shortens – a phenomenon called the windlass mechanism.
When the calf muscles contract concentrically (shorten), the Achilles tendon pulls on the calcaneus, creating tension in the plantar fascia. Elastic energy stored in the Achilles tendon and the plantar fascia is released in a coordinated manner during the push-off phase of the gait cycle, creating propulsion. The symbiotic relationship between healthy muscles, tendons and fascia is called biotensegrity. It reduces force production demands on the calf muscles, optimizing energy efficiency.
When the triceps surae and Achilles tendon are tight, they increase strain on the plantar fascia, leading to plantar fasciitis. At the same time, if the plantar fascia dysfunctions due to microtears or myofascial trigger points, foot mechanics are altered, increasing stress on the Achilles tendon and potentially leading to tendinopathy. To fully rehabilitate the Achilles tendon, we must restore biotensegrity and coordinated muscle firing patterns along the lower kinetic chain, and retrain the functional relationship between the Achilles tendon and the plantar fascia.
Age must be factored in when designing a treatment protocol. One study of cadaver feet found a gradual reduction in the number of fibers connecting the Achilles tendon and plantar fascia as humans age. A newborn has a thick continuation of fibers between the two structures, while by middle age, the foot has only superficial periosteal fibers that continue from tendon to fascia, and elderly feet show only an insertion of fibers of both structures into the calcaneus, with periosteum in between.
Rehabilitating Achilles Tendinopathy
Physical therapy alone is not enough to rehabilitate the Achilles tendon. Prior to beginning physical therapy, we pretreat the tissues to address microtears and ruptures, eliminate myofascial trigger points, and restore biotensegrity in the foot and ankle complex. Regenerative technologies, orthobiologics, and manual therapies may all be used to prepare tissues prior to loading.
Phases of Achilles tendon rehab at NYDNRehab include:
- Acute phase, aimed at reducing pain and inflammation, and protecting the tendon from further damage or degeneration. Shockwave therapy may be introduced at this phase to reduce pain and inflammation, and jump-start the healing process.
- Pre-treatment phase, where we promote tissue regeneration and begin to restore functional mobility. Orthobiologics, regenerative technologies and manual therapies come into play, with the goal of repairing and healing tissues before subjecting them to force loads.
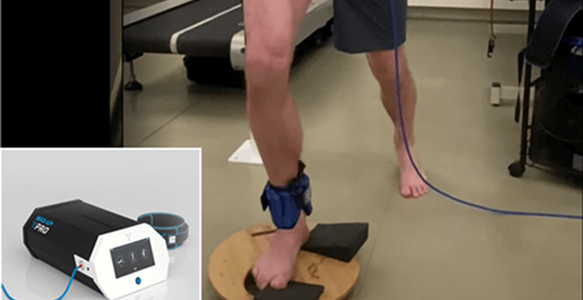
- Functional physical therapy phase, to restore joint range of motion and progressively introduce strengthening exercises. This phase includes eccentric loading, stretching, proprioception and balance, and progressive resistance training. At NYDNRehab, hamstring tendon physical therapy is personalized, based on the patient’s unique profile.
- Return-to-activity phase, to prepare the patient to return to their regular physical activities. This phase may include sport-specific skills training, plyometrics, functional drills, and enhancement of muscle coordination patterns.
We monitor every phase of your healing journey with high-resolution ultrasound. In addition to confirming tissue
healing, ultrasound imaging helps to ensure proper load
progression, and lets us monitor tissue responses to
loading.



Advanced Achilles Tendon Treatment at
NYDNRehab
Our evidence-based regenerative technologies and cutting-edge therapies are designed to accelerate healing and restore functional mobility, without drugs or surgery. Our holistic approach means your therapy will include attention paid to other tissues and structures that affect – or are affected by – your injury.

Multimodal Shockwave Therapy
Many clinics advertise shockwave therapy, but few offer radial, linear, focused and defocused shockwaves to address different tissue types. At NYDNRehab, we use ultrasound guided extracorporeal shockwave therapy (ESWT), to promote the healing of tendon and fascia tissue and restore biotensegrity. ESWT helps to realign collagen fibers, promotes hydration of the fascia tissues, and restores tissue gliding.

Ultrasound Guided Dry Needling
The dry needling procedure inserts filament-thin needles through the skin to reach myofascial trigger points – fibrous knots of tightly contracted tissues that cause pain and disrupt myofascial function. When precisely inserted, the needles cause a twitch response that immediately releases the trigger point.

PENS
Percutaneous neuromodulation (PENS) is a therapeutic approach that uses electrical stimuli to calm and desensitize hyperactivated nerves. It involves the insertion of several filament-thin needles under ultrasound guidance into muscle tissue adjacent to the targeted nerve. PENS stimulates the nerve with varying waves of low frequency electrical current to help restore optimal neural function.
Blood Flow Restriction Training (BFRT)
Rebuilding muscle strength while joints and connective tissues are still healing is a challenge for athletes who need to return to sport in the shortest time possible. BFRT enables you to increase muscle size and strength at much lower training volumes, to reduce stress on still-healing structures while rapidly restoring muscle performance. In the case of Achilles tendinopathy, BFRT can help restore strength in adjacent muscles that have atrophied due to Achilles dysfunction.

Kineo Intelligent Load System
We use the Kineo intelligent loading system to create customized training and rehabilitation programs for our patients. With Kineo, we can customize variable load protocols for functional training, core training, agility drills and more. The Kineo variable resistance system lets us design a personalized variable load curve based on the needs of the individual patient.
Orthobiologic procedures available at NYDNRehab include:







At NYDNRehab, our strategic and multifaceted approach ensures that the best procedures and methodologies are introduced at each stage of healing. We know that stand-alone solutions and one-size-fits all protocols – while they sometimes provide temporary relief – often fall short of restoring long-term functional mobility.
Knowing when and how to introduce various therapeutic approaches is an art that demands high levels of experience, skill and expertise. We combine advanced technologies and cutting-edge therapies with tried-and-true techniques that produce lasting results. Our track record of success makes NYDNRehab the premier clinic for Achilles tendon rehabilitation in NYC.
Preventing Achilles Tendinopathy
There are several things you can do to reduce your risk of Achilles tendon injuries:
- Optimize your nutrition for protein and collagen synthesis. Bone broth and collagen supplements provide the fundamental building blocks for post-exercise tendon recovery. High-quality protein from grass-fed, pasture-raised and wild-caught beef, poultry and fish are the best sources of amino acids essential to muscle and tendon repair.
- Drink plenty of water. Dry tendons are less elastic and more likely to rupture.
- Choose supportive footwear that provides stability shock absorption, and frequently replace worn athletic shoes.
- Gradually increase training and activity levels to avoid overuse.
- Avoid sudden changes in training intensity or training surface.
- Stretch and strengthen the calf muscles on a regular basis.
- Maintain a healthy weight to reduce tendon stress.
- Avoid corticosteroid injections, which can degrade tendon tissue.
- Get a biomechanical analysis to trouble-shoot and retrain faulty biomechanics.
- Allow for ample recovery time after sports and exercise, especially if you have delayed-onset soreness. Most people need at least 48-72 hours to recover from intense physical activity.


Range of Available Unique Physical Therapy
Treatments at Nydnrehab
Achilles Tendinopathy FAQs
Several factors can increase your risk of Achilles tendinopathy, including:
- Repetitive overuse from sports and exercise.
- Sudden increases in training intensity, frequency, and/or duration.
- Tight calf muscles and poor flexibility.
- Inefficient training technique.
- Worn or inappropriate footwear.
- Reduced tendon elasticity due to aging.
- Medications like steroids, statins and fluoroquinolone antibiotics.
- Obesity and metabolic disorders.
The rate of recovery can vary, depending on various factors:
- Location of the injury (insertional or non-insertional
- Severity of ruptures and tissue damage
- Degree of tissue degeneration
- Training status
- Health, nutrition, and other lifestyle factors
- Medications
- Quality and type of treatment received
- Compliance with the rehab protocol
Mild cases of Achilles tendinopathy may improve within 6–12 weeks with consistent treatment, while chronic and severe cases can take 3–6 months or longer.
Adherence to physical therapy and avoiding reinjury are key to recovery.
Pain that persists or worsens, despite rest and basic first aid, is an indication that you may need professional attention. Sudden severe pain can indicate a tendon rupture, which needs to be quickly treated. Swelling, deformity, and difficulty walking or standing on your toes are all indicators that you need help.
Tendinopathy involves tendon degeneration or microtears in tendon tissue, while a rupture is a complete or partial tear of the tendon. Tendinopathy is painful, but not completely debilitating, while a tendon rupture is marked by sudden intense pain and loss of function. Severe ruptures may require urgent care or surgery.
Always follow the advice of your sports physical therapist. Some low-intensity activities like swimming or cycling may be okay if they don’t cause pain, but you should avoid high-impact activities that involve running or jumping until your symptoms improve.





















