
Hip Labrum Pain and Dysfunction
Personalized boutique services supported by cutting-edge integrative diagnostics and advanced holistic therapies.
Dr. Kalika and Dr. Brosgol are Raising
the Bar on Hip Labrum Therapy
Clinical director & DC RMSK
Verified Expert Profiles
Dr. Lev Kalika, DC, RMSK, clinical director and founder of NYDNRehab, is an expert in integrative physical rehabilitation with over 20 years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. He is an active member of the American Institute of Ultrasound in Medicine (AIUM), and his expertise in diagnostic ultrasonography is recognised by his peers on the world stage, where he frequently presents his own research on ultrasound-guided procedures.
Dr. Kalika is the only clinician in New York certified by the International Society for Medical Shockwave Therapy (ISMST) to perform extracorporeal shockwave therapy. He has developed his own unique approach to dynamic functional and fascial ultrasonography and has published peer-reviewed research on the topic. Dr. Kalika is a specialist in orthobiologics, a certified practitioner of Stecco Fascial Manipulation, and an esteemed member of multiple professional organizations.

Dr. Yuri Brosgol specializes in advanced ultrasound-guided regenerative medicine for the non-surgical treatment of musculoskeletal pain, osteoarthritis, and sports injuries. His clinical approach includes prolotherapy, neuroprolotherapy, PRP injections, and stem cell-based procedures. His expertise and years of clinical experience inform his selection of personalized procedures, based on specific tissue pathology and individual patient profiles.
Dr. Brosgol’s holistic orthobiologic approach goes beyond injection therapy – he factors in biomechanics, inflammation, nerve irritation, recovery potential, and systemic contributors to healing. His background in functional medicine equips him to successfully treat patients with complex, chronic, or recurrent musculoskeletal conditions.
Patients seeking alternatives to surgery, active individuals with osteoarthritis, athletes with overuse or sports injuries, and patients who have not improved with conventional treatment can all benefit from Dr. Bosgol’s expertise.
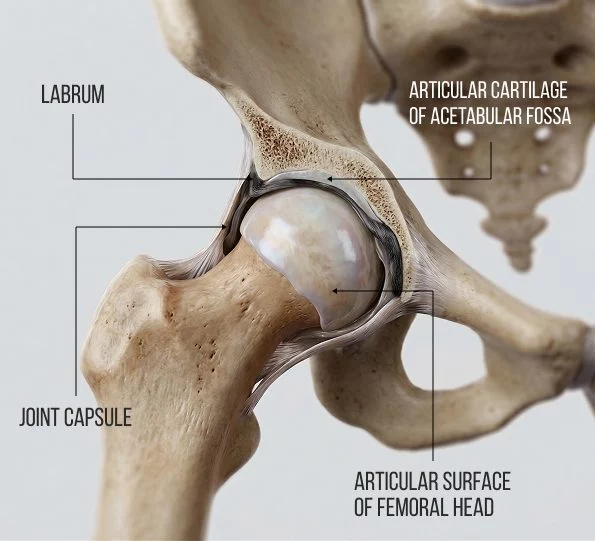
Functional roles of the acetabular labrum include:
- Hip stabilization – the labrum deepens the hip socket by 30% and increases its volume by 20%, covering the femoral head and dramatically improving stability.
- Creates a suction seal – by creating negative intra-articular pressure and maintaining a film of synovial fluid between the femoral and acetabular cartilage, the labrum holds the femoral head in place and reduces friction.
- Helps to distribute force loads across the joint and provides shock absorption.
- Contributes to proprioception and pain generation – the capsular side of the labrum is richly innervated with free nerve endings and mechanoreceptors, making labral tears a major source of mechanical hip pain.
- Preserves a fluid seal, protecting the joint cartilage from excessive stress.
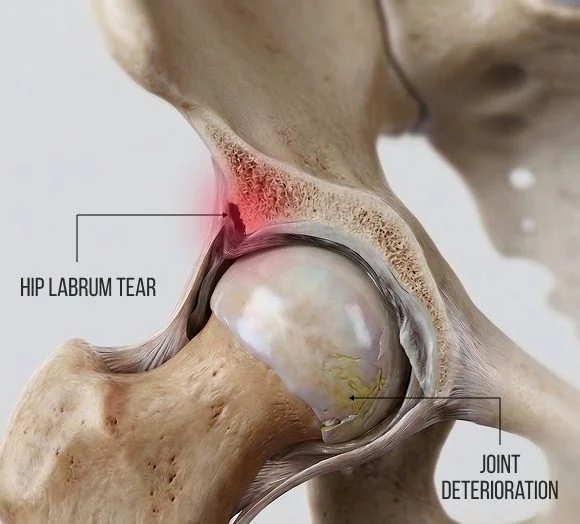
Labral Tears Disrupt Hip Mechanics
Labral tears typically arise from acute trauma from an accident or sports injury, or from repetitive microtrauma due to overtraining, causing subluxation or dislocation of the hip and damaging the labrum. Up to 90% of labral tears occur in the anterosuperior segment, where FAI injuries are most common.
- Traumatic events, such as a hard hit, fall, or a high-impact twisting injury.
- Femoroacetabular impingement (FAI) – the most common type of labrum injury – where the labrum is pinched between the acetabulum and the femoral head.
- Capsular laxity, where joint stability diminishes, causing increased pressure on the labrum and resulting in wear and tear.
- Dysplasia, where a bony abnormality in either the acetabulum or the femoral head increases stress on the acetabulum and/or the labrum.
- Degeneration, where the labrum, cartilage and bone begin to deteriorate.

Conventional hip labrum treatment involves activity modification, anti-inflammatory medications, corticosteroid injections. and conventional physical therapy. But those measures often fall short of fully restoring functional mobility, leaving patients with surgery as their only remaining option.
Traditional hip labrum surgery involves debridement, where an arthroscopic procedure is performed to remove or smooth out torn and frayed cartilage. While the procedure may temporarily relieve pain, debridement can have negative long-term effects on hip joint function. Debridement reduces the joint depth by up to 30%, severely impairs the suction seal, interferes with load distribution, increases friction, and accelerates the rate of osteoarthritis.
Today, new advancements in integrative medicine are transforming the way hip labrum tears are diagnosed, evaluated and treated, restoring and preserving the protective properties of the acetabular labrum without invasive surgery.
Diagnosing Hip Labrum Dysfunction
Diagnosis of the hip labrum begins with a health history, followed by a clinical exam. The exam will most likely include a FADIR (Flexion-Adduction-Internal Rotation) assessment, which is essentially a test for anterior labral impingement. The FADIR has a high rate of sensitivity, with high confidence in up to 99% of cases.
In addition, your diagnostic protocol may include ForceFrame, a comprehensive system for accurately testing and training isometric strength. In the case of hip labrum dysfunction, ForceFrame lets us assess and compare differences in muscle strength between the affected and unaffected hip, a key indicator of hip labrum disorders. The results also provide a baseline for measuring progress in response to treatment.
At NYDNRehab, we confirm the findings of our clinical exam with the highest-resolution ultrasonography currently available. Your ultrasound exam takes place on your first visit, in the comfort of our clinic. Research shows that while high-resolution ultrasound is slightly less sensitive than MRI for detecting labral tears, it has a higher sensitivity and predictive value overall.
Ultrasound is less expensive, faster, and more convenient than MRI for evaluating anterosuperior acetabular labral tears, with the overriding advantage of dynamic real-time imaging. Dr. Kalika’s skill in interpreting diagnostic ultrasound imaging, combined with his in-depth knowledge of human anatomy and musculoskeletal pathology, have earned him international recognition among his peers in the integrative medicine community.

Physical Therapy Alone Cannot
Restore a Torn Hip Labrum
While physical therapy can be useful post-treatment to help restore strength, stability and functional mobility, it cannot re-create a damaged acetabulum’s suction seal or restore its capacity for load distribution. At the same time, while surgery can offer temporary pain relief, it cannot restore the acetabellum’s functional properties, leaving patients with little hope for full recovery.
The hip labrum has very low vascularity, limiting its ability to self-heal – especially the superior/anterior portion where most tears occur. But new regenerative technologies and therapies are redefining how hip labrum dysfunction is assessed and treated. This approach requires a personalized, multifaceted framework based on the patient’s unique profile, and demands the skill and expertise of a trained integrative specialist.
Many physical therapy clinics offer regenerative energy and injection therapies to their patients, but lack the experience and skill to use them effectively. Therapies delivered without high-resolution imaging are hit-or-miss at best, often failing to provide any relief of symptoms, and prolonging the patient’s pain and dysfunction.
At NYDNRehab, we guide all or our regenerative procedures with high-resolution ultrasound, ensuring precise targeting of specific tissues without the risk of penetrating nerves and blood vessels. Dr. Kalika and Dr. Brosgol work as a team, combining their expertise to optimize patient outcomes. Only when tissues are healed and ready to bear loads do we introduce physical therapy to restore functional mobility.

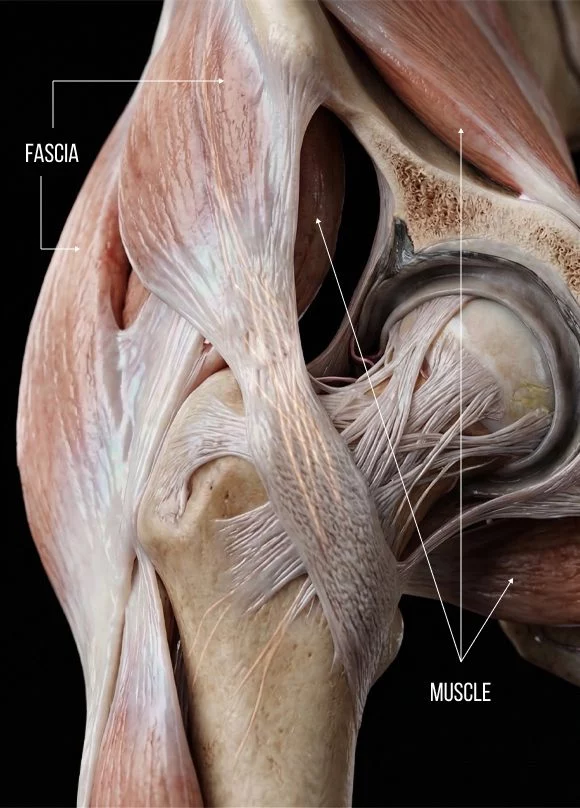
The Role of Fascia in Hip Labrum
Mechanics
Fascia is a thin tough network of collagenous tissue that connects and surrounds the body’s tissues and anchors vital organs in place during movement. Fascia works hand-in-hand with muscle, forming the myofascial system that guides, controls, and distributes internal and external forces via a continuous state of elastic tension called biotensegrity.
Until recently, fascia was considered a non-essential tissue that was often discarded during cadaver research. But today, fascia research has exploded as scientists become aware of its crucial role in biomechanics. Its slippery and elastic properties allow for smooth gliding of nerves and blood vessels among larger structures, and its capacity for proprioception plays a critical role in kinesthetic awareness and pain generation. The most recent research has discovered that fascia has contractile properties, once thought to be the domain of muscle tissue alone.
Fascia has a substantial influence on hip labrum mechanics, coupling with the labrum’s surrounding myofascial and ligamentous systems. When fascia becomes densified or forms adhesions, load transfer to the labrum is directly altered, which can lead to pain, dysfunction, and tearing.
The iliofemoral ligament – provides the strongest fascial restraint, preventing the hip from over-rotating and excessive extension.
The deep gluteal fascia and the piriformis-obturator internus complex – this dense fascia encases the sciatic nerve and deep hip rotators. Restrictions from this fascia are common in dancers, yoga practitioners, and people who sit with hips flexed at 90 degrees for extended periods of time.
The iliotibial band (ITB) and tensor fasciae latae (TFL) that form the iliopsoas continuum – a tight TFL/ITB pulls the femur into relative external rotation and abduction, overloading the posterosuperior labrum, a condition commonly seen in runners.
The thoracolumbar fascia, impacting the quadratus lumborum, psoas, and anterior capsule chain – dysfunction of this fascia can cause lumbopelvic stiffness, leading to anterior pelvic tilt and increased lumbar lordosis, resulting in chronic labral overload.
The pubofemoral and ischiofemoral ligaments – tightness in these structures can cause inferior fascial restrictions that limit abduction and external rotation, increasing compressive load on the superior labrum.
Regenerative Therapies Surpass Surgery
for Hip Labral Repair
NYDNRehab is at the cutting edge of regenerative therapies, using the most advanced technologies and highest-quality solutions available. Regenerative therapies include energy technologies and injectable orthobiologics, frequently used in combination to obtain a synergistic effect.
All of our regenerative procedures are guided by high-resolution ultrasound to ensure precise targeting and avoid accidental penetration of neurovascular bodies.
Orthobiologics use blood platelets, bone marrow and adipose derivatives, extracted from the patient’s own body and highly concentrated. When injected into damaged tissues, they stimulate a regenerative healing response that accelerates recovery. At NYDNRehab, we offer a broad range of injection therapies to optimize results.









Energy technologies use sound, light, radiofrequency, and electromagnetic pulses to reduce pain and inflammation, and stimulate a regenerative response, By carefully selecting and combining the most appropriate therapies, we are able to harness the synergistic effects of both energy technologies and orthobiologics, for superior and enduring results. Depending on the individual patient case, energy technologies may be used before or after your injection, or both.



Common mechanical issues that cause hip labral stress include:
- Densified fascia that interferes with muscle action and restricts load transfer.
- Repetitive overuse that stresses the labrum and creates muscle imbalances.
- Asymmetrical motor patterns in certain sports and occupations that cause misalignment.
- Injuries or mechanical dysfunction further along the kinetic chain.
- Tight hip flexors and weak glutes from too much sitting.
Personalized physical therapy helps to strengthen supporting structures, balance myofascial tension, improve biomechanics, and correct poor posture. For athletes and physically active people, physical therapy can help to improve performance and reduce your risk of future injuries. Beware of clinics that offer regenerative therapies without addressing the myofascial system’s role in hip labrum pathology.
Preventing Hip Labrum Injuries
Injuries to the hip labrum can be prevented by proactively optimizing the function of the lumbopelvic/hip complex. Follow these tips to protect your hips.
- Adopt a progressive training routine to build hip stability and motor control. Choose exercises that target the deep hip stabilizers (gluteus medius/minimus, deep external rotators, iliopsoas).
- Avoid exercises that overstretch and load the anterior labrum, like deep lunges, or aggressive yoga poses like pigeon.
- Gradually increase your training volume for sports that involve cutting, pivoting, or deep hip flexion, such as soccer, hockey, dance, and Olympic lifting.
- Strengthen your entire kinetic chain, including core, feet and ankles that directly affect hip mechanics and force transfer.
- Maintain a healthy body weight and avoid excessive sitting.


Get State-of-the-Art Hip Labrum Treatment in NYC
Choosing a physical rehab center from the dozens located in Manhattan can seem overwhelming, but you can quickly narrow down your options by asking a few pertinent questions:

- What are the credentials, experience, and expertise of the specialists, and do they have a successful track record? At NYDNRehab, Dr. Kalika and Dr. Brosgol are seasoned integrative practitioners, with years of hands-on clinical experience and a proven record of successful patient outcomes.
- Do they offer customized treatment protocols? At NYDNRehab, we treat the whole patient, not just your symptoms. Our personalized approach ensures that you get the exact treatment you need, based on the unique characteristics of your condition. We never use generic one-size-fits-all protocols, and our treatment sessions are one-on-one.
- What is their diagnostic approach? When based on symptoms alone, diagnosis is hit-or-miss, and patients often receive inappropriate or ineffective treatment. In addition to a clinical exam and diagnostic testing, we conduct a high-resolution ultrasound exam on your first visit, to confirm our findings and identify hidden issues.
- What therapies and interventions are available? The clinic at NYDNRehab features some of the most advanced technologies and therapies available in integrative medicine. Our commitment to quality and precision, and our multimodal treatment protocols ensure you get the best possible therapy, for fast, effective, and lasting recovery.
When it comes to getting state-of-the-art treatment for hip labrum disorders, your choice is a no-brainer. NYDNRehab is Manhattan’s premier clinic of choice for physical rehab in NYC.
Our Awards





Real Patient Cases Treated at NYDNRehab
These case studies reflect real clinical conditions evaluated at NYDNRehab using advanced diagnostic methods and individualized rehabilitation strategies. All cases are evaluated and managed by Dr. Lev Kalika and the NYDNRehab clinical team.
Hip Labrum FAQs
The hip labrum deepens the socket where the head of your femur fits into your pelvis, making your hip more stable. It functions as a seal for synovial fluid, keeping it inside the joint to prevent friction and nourish joint tissues. The labrum plays a key role in absorbing shock and distributing force loads during physical activity.
With rest and rehab, small stable tears in the outer, more vascular region can self-heal. But tears in the anterior-superior region where blood supply is limited are unlikely to heal on their own. Regenerative therapies can successfully stimulate healing in avascular tissues when correctly applied.
When incorporated into a strategic, multimodal treatment protocol, physical therapy plays a key role in recovery, but physical therapy alone cannot reattach or heal a torn labrum.
Only between 25-35% of labral tears require surgery. Surgical options are usually reserved for cases where the hip is catching or locking, or when no progress is made after months of physical rehab. Surgery may be called for in cases where FAI or dysplasia is causing the joint to degenerate.
No, they are two separate conditions. FAI occurs when the labrum is pinched in the antebellum. It can lead to tearing if left untreated. You can have FAI without a tear, and you can have a tear without FAI.





















