To physically function and perform at your peak, you need joints that are both mobile and stable, and capable of withstanding force loads multiple times your body weight. Joint hypermobility syndrome (JHS) is a hereditary condition where lax ligaments allow the joints to extend beyond their optimal functional range of motion. Joint hypermobility is a key symptom of Ehlers Danlos syndrome (EDS), a set of connective tissue disorders caused by defects in collagen structure and production.
Dancers, gymnasts and acrobats may benefit from hypermobile joints, but people with JHS and EDS often suffer from physical instability and a higher-than-average risk of injury. Specialized physical therapy can help improve joint stability by strengthening the structures that support hypermobile joints, and by equipping patients with effective strategies for managing their condition.
Clinical director & DC RMSK
Verified Expert Profiles

Orthobiologic specialist
Dr. Yuri Brosgol, MD is a neurologist with 20+ years of experience in treating pediatric and adult myofascial pain. When emerging research on the critical role of fascia in human mobility captured Dr. Brosgol’s interest, he pursued training in orthobiologics and fascial release techniques. Dr. Brosgol has become a pioneer in the use of orthobiologic solutions and fascial plane hydrodissection, paving the way for transformative advancements in the treatment of myofascial disorders.
Together, Dr. Kalika and Dr. Brosgol are combining their skills to revolutionize the way myofascial pain is diagnosed and treated. By leveraging the most advanced, evidence-based approaches, they are dedicated to improving the quality of life of JHS/EDS patients in NYC.
Joint hypermobility syndrome is a genetic condition characterized by joints that move beyond their normal range of motion. JHS patients often report chronic joint pain, fatigue, and frequent soft tissue injuries like sprains or dislocations. JHS is thought to be related to lax ligaments and tendons, and irregular collagen fiber arrangement in connective tissues.
Symptoms of joint hypermobility syndrome include:
Unlike JHS which is mostly isolated to connective tissues at the joints, EDS has a broader scope, often affecting multiple systems including joints, skin, blood vessels, and organs. EDS is associated with genetic mutations that cause defects in collagen – a protein that serves as a primary building block for the body’s connective tissues, affecting skin, bones, tendons, ligaments, and cartilage. EDS symptoms are typically more severe than those of JHS, and some can be life-threatening.
Symptoms of EDS vary from one type to another, and may include:
When faced with joint hypermobility, most physical therapy clinics rely on one-size-fits-all exercise protocols, with the goal of strengthening the structures that stabilize the joints. But advancements in research show that muscle and tendon strengthening is not enough to reduce symptoms, improve joint function, and enhance physical performance in JHS patients.
At NYDNRehab, we treat the whole patient, not just your symptoms. We not only address the structural stability of joints – we use dynamic ultrasound imaging and advanced diagnostics to discover other factors that contribute to joint dysfunction. Ultrasound lets us visualize the body in motion, in real time, to see how the various structures interact, and equips us with sonoelastography to test tissue stiffness.
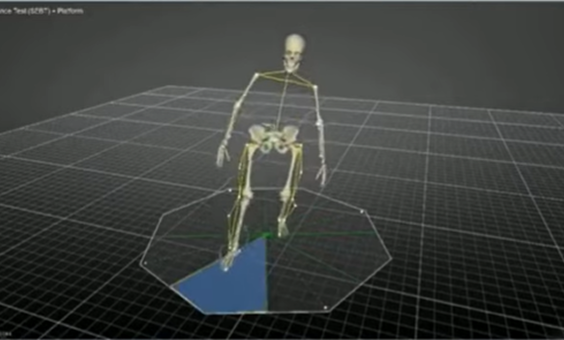
Our state-of-the-art motion analysis lab and proprietary software give us objective data about critical movement parameters that govern joint mobility and stability. With these insights, we are able to create personalized treatment protocols, customized to the patient’s specific needs.
Our revolutionary approach to joint hypermobility disorders makes NYDNRehab the clinic of choice in NYC for JHS/EDS diagnosis and treatment.

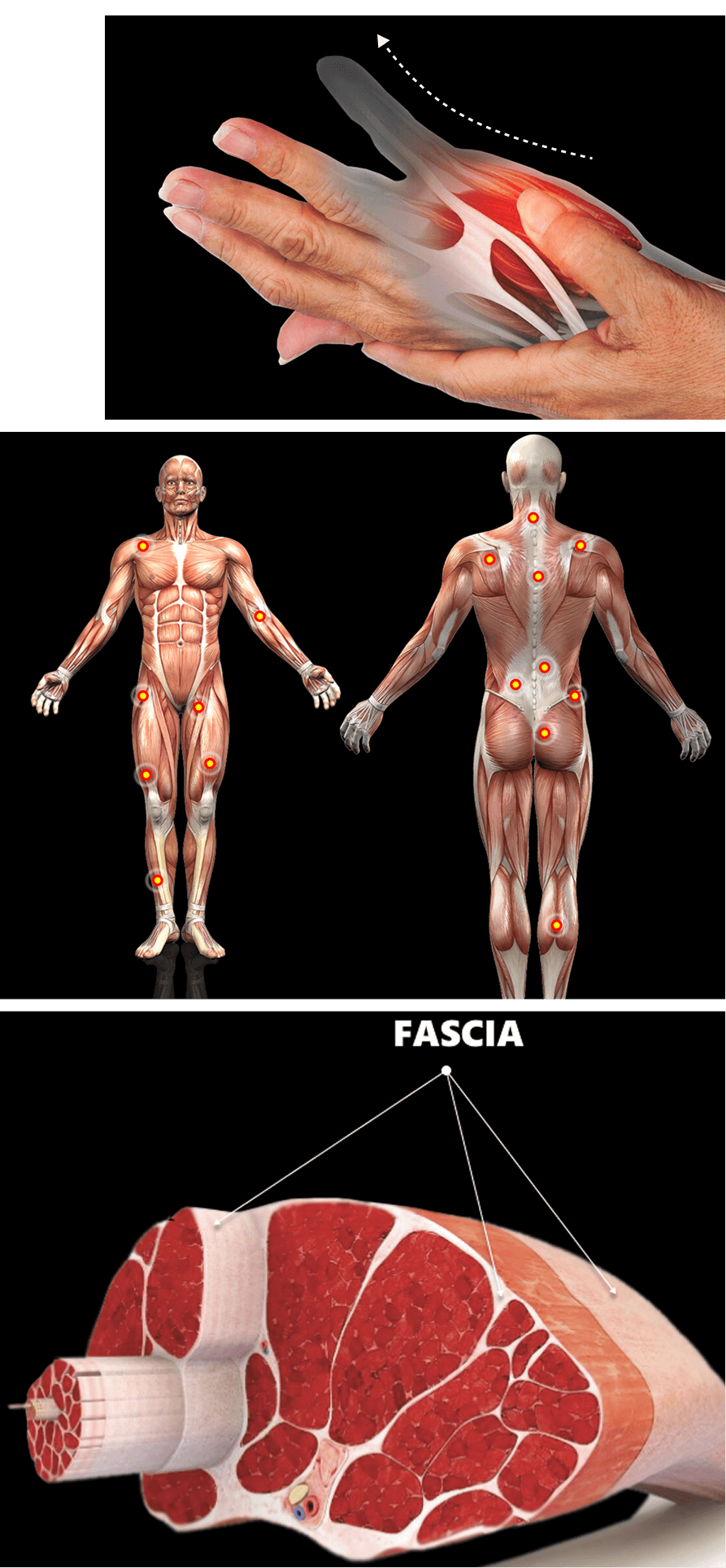
Fascia is a thin fibrous web of connective tissue that separates, connects and encases muscles, joints, organs, nerves and blood vessels throughout the body. It works together with muscles to guide and control movement by providing tensegrity – elastic tension that holds structures in place as you move.
Fascia is primarily made up of collagen, elastin, and a gel-like substance composed of hyaluronic acid and water. Fascial tissue is tough, elastic and slippery, allowing it to stretch and glide among the body’s structures without friction. Fascia is dynamic and adaptable, but when injured, inflamed or dehydrated, it can lose its functional properties, causing pain and inhibiting mobility.
Fascia is richly embedded with proprioceptors – specialized sensory receptors that provide the nervous system with information about the position, movement, and tension of joints – serving as a communication pathway between different parts of the body. Thanks to proprioception, you can perceive your body’s position, motion, and equilibrium without visual input.
Myofascial pain is a common symptom in JHS patients. Recent research suggests that damaged fascia may be an important factor that causes pain and inhibits mobility in JHS patients. When damaged, fascia can become dense and sticky, losing its elasticity, adhering to other structures, and entrapping nerves and blood vessels in its layers.
Damage to fascia can disrupt proprioception, leading to reduced accuracy in signaling that causes the brain to misinterpret information about the body’s spatial position, such as joint angles or muscle tension. This can cause balance issues, poor muscle coordination, and compensatory motor patterns that increase injury risk. Damaged fascia can also heighten pain signaling due to nerve compression.
Research shows that when fascial gliding is restored, it improves motor unit recruitment patterns and wakes up dormant and inhibited muscle stabilizers. Dr. Kalika specializes in myofascial release techniques that restore the elastic and slippery properties that enable fascial gliding. This critical step is often missing in conventional JHS physical therapy, resulting in failed attempts to relieve pain and improve joint stability.
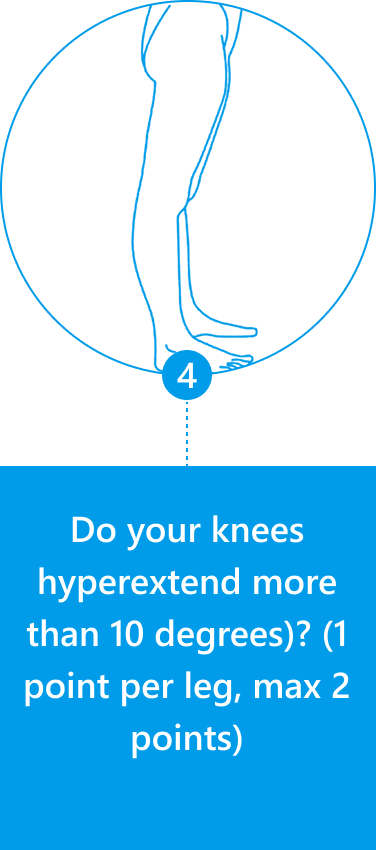
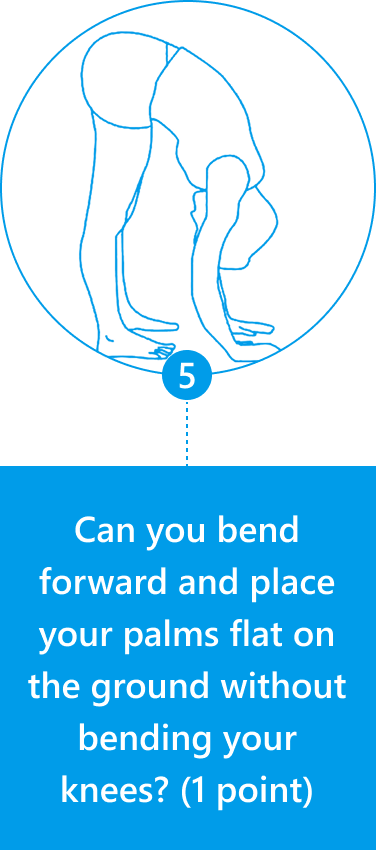
Diagnosis of JHS is mostly joint-focused and symptoms-based, while hypermobile EDS (hEDS) often involves skin, organs, and other tissues. In both JHS and hEDS, diagnostic criteria are based on the Beighton Score — a diagnostic tool for joint hypermobility that assesses joint flexibility in 5 areas of the body, with a maximum score of 9 – the higher your score, the greater your joint laxity.
You can use the Beighton Score to assess your own joint mobility:
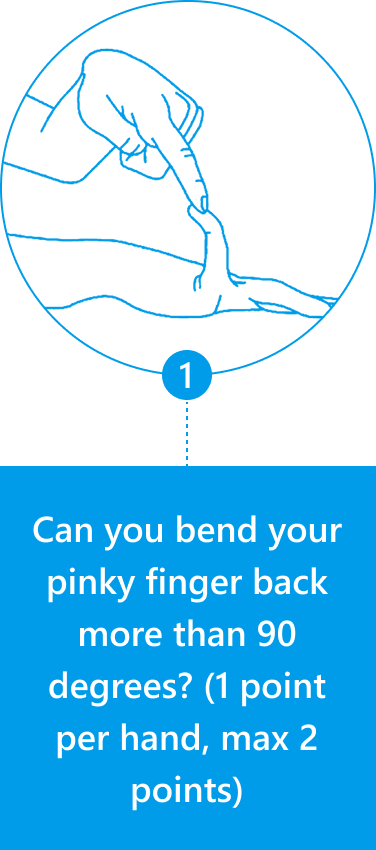
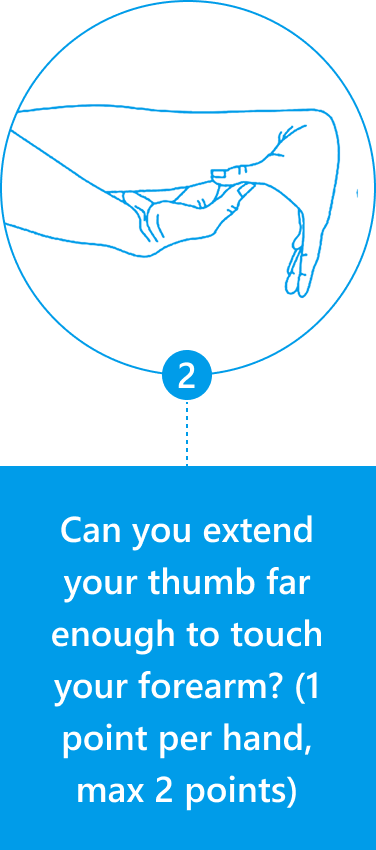
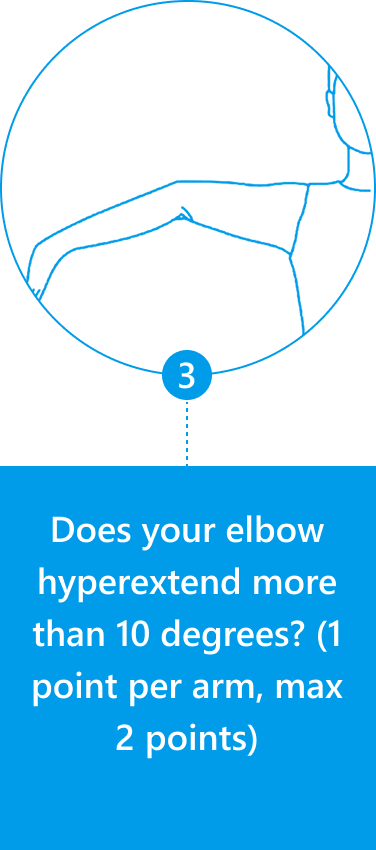
Clinicians typically use the Beighton Score along with other diagnostic criteria, such as reported symptoms of skin hyperextensibility, tissue fragility, chronic pain, and family history
NYDNRehab is one of the few private clinics to feature high resolution musculoskeletal ultrasonography. When used as a diagnostic tool, ultrasound lets us visualize the body's tissues and structures in motion, to observe how they interact. With real-time imaging, we are able to identify damaged fascia, detect entrapped nerves and blood vessels, and observe inefficient muscle recruitment patterns that contribute to JHS pain and dysfunction.
At NYDNRehab, we use ultrasound elastography – a specialized imaging technique that measures both the thickness and stiffness of deep fascia. In hypermobility disorders, deep fascia is often thicker than normal, and less stiff, indicating changes to connective tissues that characterize JHS and hEDS. Sonoelastography equips us with an advanced diagnostic tool that provides insights leading to a more accurate diagnosis, resulting in more targeted and effective treatment.
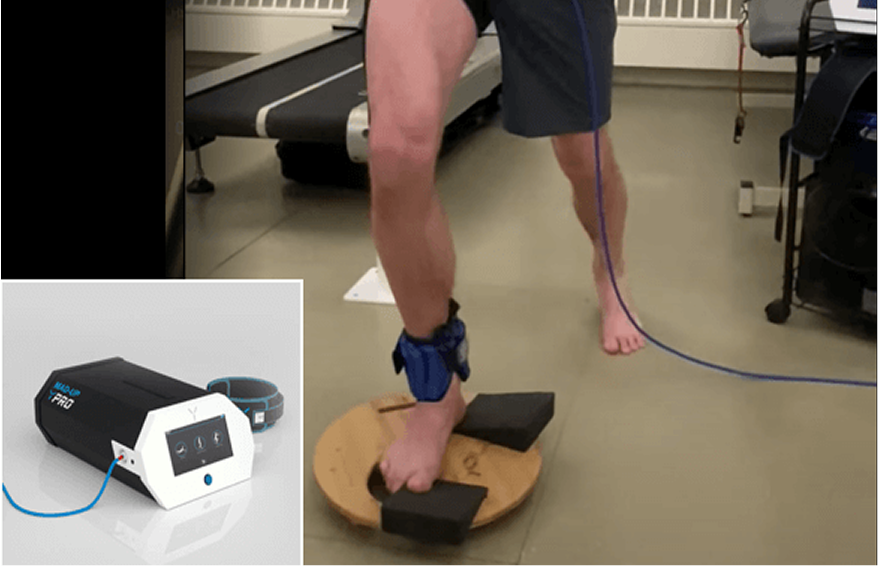
We use advanced technologies for objective and comprehensive analysis of the stability of the lower kinetic chain. These tests provide insight into how the patient's muscles, joints, and connective tissues work together to provide support, control movement, and prevent injury, helping us to customize the treatment protocol.
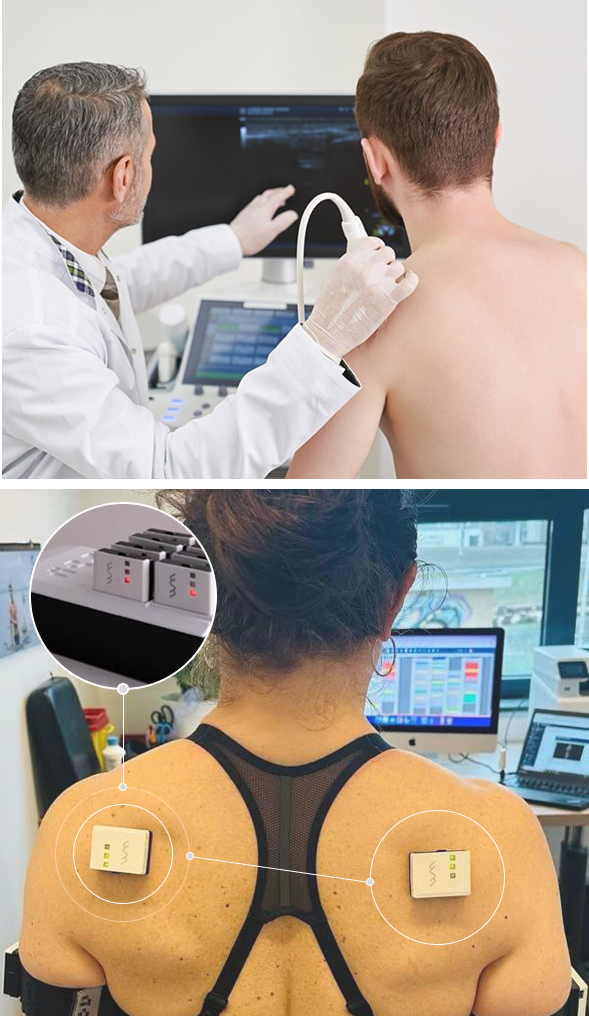
Imaging of the scapula using high-resolution ultrasound is an important tool for observing how the scapula moves relative to the humeral head of the shoulder joint. Accurate interpretation requires a skilled clinician with a comprehensive knowledge of human anatomy. Combining scapular ultrasound with ShowMotion technology provides substantial information for comprehensive shoulder rehabilitation.
Scapular imaging is especially useful for patients with rotator cuff tears, joint hypermobility syndrome (JHS), or Ehlers-Danlos syndrome (EDS) whose joints are prone to excessive movements and instability. In such cases, the connective tissues surrounding the shoulder joint tend to be lax and weak, causing poor joint stability and increasing the risk of shoulder subluxation/dislocation.
The scapula compensates for shoulder instability by acting as a stable base for positioning the glenoid fossa, to optimize positioning of the humeral head. Dynamic scapular stabilization requires well-coordinated muscle activation patterns, especially of the rotator, deltoid, trapezius and rhomboid muscles. Scapular dysfunction can increase strain on the rotator cuff and labrum, contributing to pain and instability.
Dynamic scapular imaging lets us observe the complex interactions of the shoulder girdle kinetic chain, to pinpoint issues such as deficiencies in muscle activation, glenohumeral joint subluxation, and capsular laxity that contribute to shoulder instability. For patients with rotator cuff tears , JHS/EDS patients, scapular ultrasound can be a game-changer, ensuring they receive proper rehabilitation that enhances stability after a shoulder dislocation.
Thanks to advanced technologies and regenerative therapies, there are new and innovative treatment options for JHS/EDS, but you won’t find them at most physical therapy clinics. NYDNRehab is one of the few private clinics in NYC where you can access a wide array of evidence-based advanced therapies for JHS treatment.







Ligaments are tough fibrous connective tissues that attach bones to bones, providing joint stability. Ligaments are not very elastic, and their length is more-or-less fixed in adults. But otherwise-normal joints can become hypermobile when subjected to injury or repeated stress. For example, an ankle sprain can cause ligaments to stretch or tear, creating ankle instability.
Activities like yoga, ballet, gymnastics and acrobatics whose training includes extreme stretching can lengthen ligaments, causing joint hypermobility and instability. Balancing those activities with strengthening exercises like resistance training can help to preserve ligament integrity and provide additional joint support through stronger muscles and tendons.
By contrast, JHS and DHS are hereditary conditions that cannot be prevented – only managed. Specialized physical therapy can help to increase strength, promote balance and coordination, and build confidence in hypermobility patients. Activities like swimming and water exercise can help to strengthen and stabilize joints without serious risk of injury. Optimizing lifestyle behaviors can improve overall health, reducing the burden of managing hypermobile joint disorders.


Despite their best intentions, conventional approaches to treating joint hypermobility have a poor track record of success. In fact, traditional physical therapy can actually make the condition worse. Most therapists lack the training or expertise to effectively address JHS/EDS, and pain management efforts like steroid injections do not produce long-term relief. Surgery is often recommended as a last resort, but surgery for EDS has a high rate of failure.
At NYDNRehab, our unique and comprehensive approach is based on years of experience and continuing education in advanced methodologies. Dr. Kalika and Dr. Brosgol are pioneers in cutting-edge therapies that are changing the game in rehabilitative medicine, providing new hope for JHS/EDS patients.





























Independent peer-reviewed research relevant to this treatment approach.

Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination