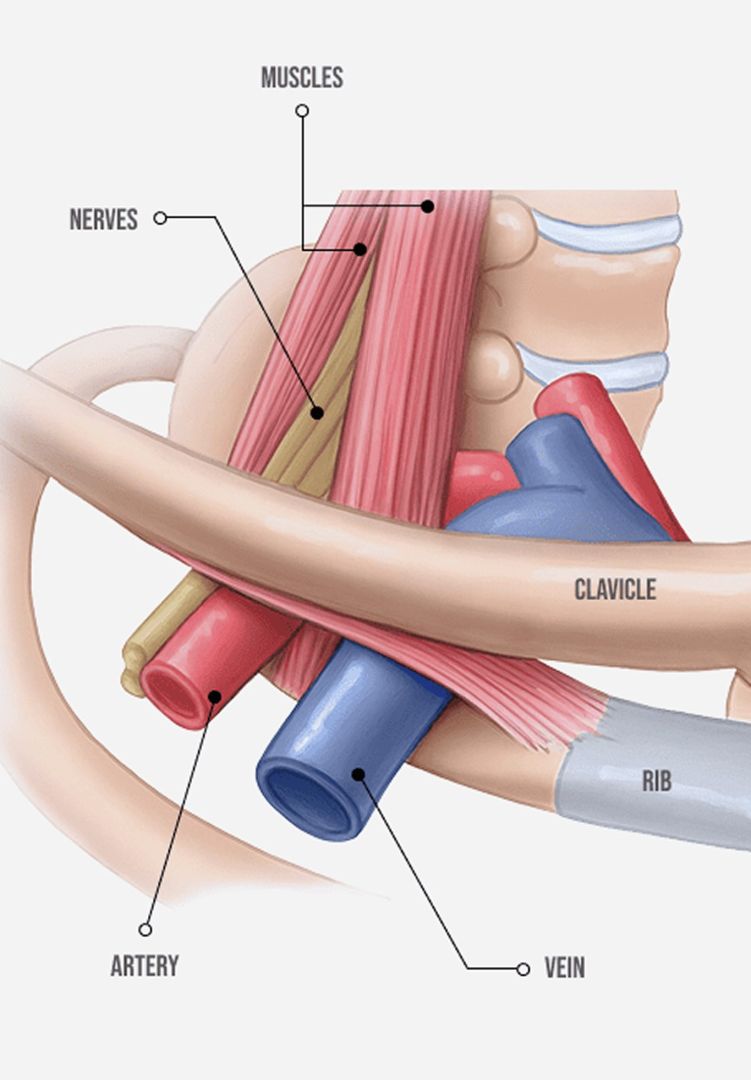
The thoracic outlet is a narrow passage located just above the first rib and behind the clavicle, near the base of your neck. It provides a space for nerves (brachial plexus) and blood vessels (subclavian vein and artery) to travel from your chest to your arm. Due to multiple factors, this already-crowded passageway can narrow, compressing the neurovascular bundle, producing pain, and inhibiting blood flow — a condition called thoracic outlet syndrome (TOS).
While technically not a shoulder condition, thoracic outlet syndrome is affected by shoulder mechanics. TOS is common in athletes who participate in overhead sports like swimming, tennis and baseball, and in certain occupations that require overhead movement, like house painting or plaster work. TOS can also arise from weak muscles and poor posture that alter the position of the clavicle.
If left untreated, TOS can cause blood clots and pulmonary embolisms, and long-term TOS can lead to permanent nerve damage. At NYDNRehab, advanced technologies, orthobiologics and holistic methodologies are redefining how thoracic outlet syndrome is diagnosed and treated.

Clinical director & DC RMSK
Verified Expert Profiles
Dr. Lev Kalika, DC clinical director of NYDNRehab, is an internationally recognized expert in diagnostic and musculoskeletal ultrasonography, with multiple research papers to his credit. Dr. Kalika has studied with some of the world’s most prestigious experts in diagnostic, fascia, and nerve ultrasonography, including Dr. Ben Kibler, world-renowned orthopedic surgeon and pioneer of scapular dyskinesis. Dr. Kalika has published multiple peer-reviewed studies on ultrasound-guided procedures, and has presented his research at multiple international conferences.

Orthobiologic, Sports Medicine and Regenerative Medicine Specialist
The thoracic outlet is a space formed at the junction of your neck and shoulder that houses vital structures like the brachial plexus (nerves to the arm and hand), the subclavian artery that feeds your arm, and the subclavian vein that returns deoxygenated blood from your arm to your heart. The esophagus and trachea also pass through the thoracic outlet.
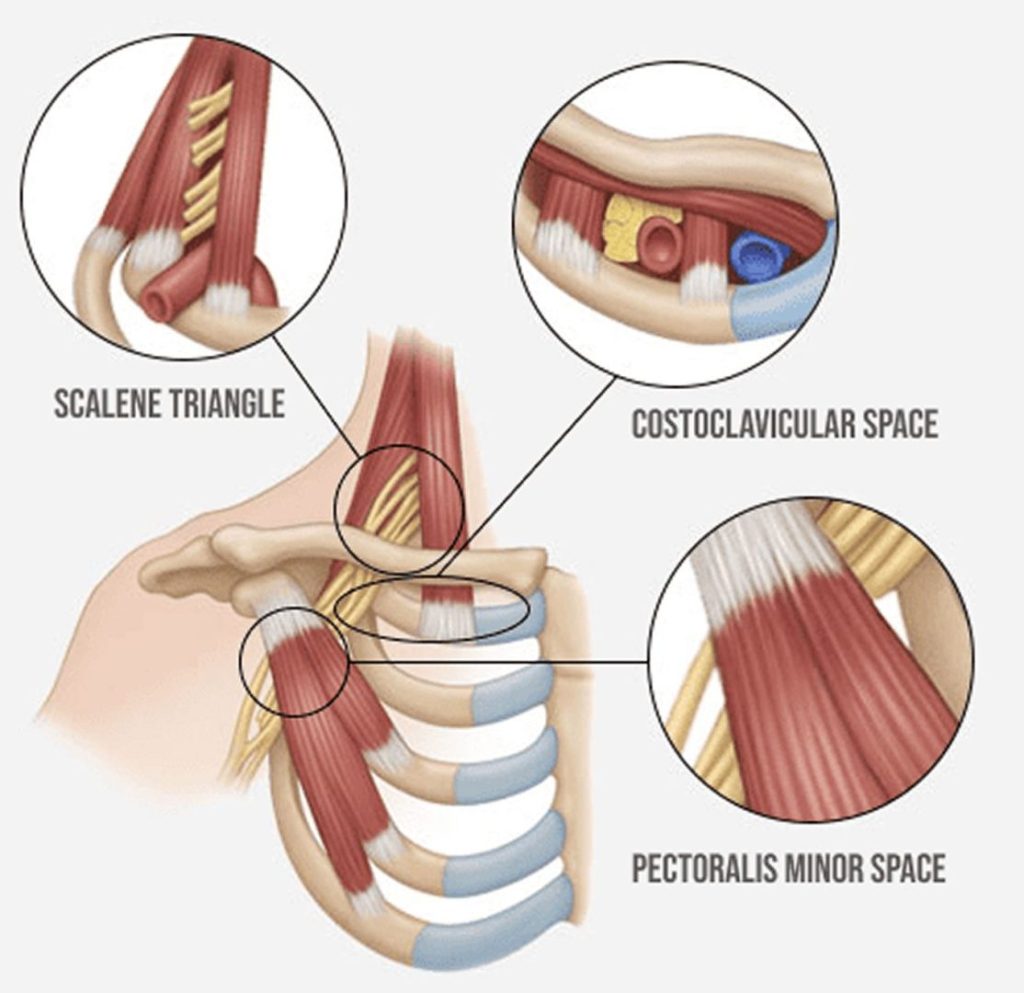
The nerves that form the brachial plexus emerge from the spinal cord in the neck and pass between the anterior and middle scalene muscles, responsible for forward and lateral neck flexion, head and neck rotation, and rib elevation when breathing. Tight scalene muscles, along with tight pectoral and deltoid muscles, can all contribute to compression of the brachial plexus within the thoracic outlet.
While TOS in athletes is strongly associated with overhead sports like swimming and tennis, other factors can contribute to TOS in non-athletic populations.

Most TOS cases can be successfully treated with holistic interventions and lifestyle modifications. Surgical options are extreme, such as scalene muscle release, where the scalene muscles are cut or partially removed to relieve pressure on the brachial plexus, or first rib resection, where part or all of the first rib is removed. TOS surgery can have serious potential complications including bleeding, nerve injury, pneumothorax (from first rib resection), and recurring symptoms post-surgery.
Dr. Kalika has developed his own holistic methodology for diagnosing and treating conditions of the neck, shoulder and brachial plexus, using cutting edge kinematic motion analysis technology and dynamic ultrasound imaging. In addition to identifying the subtype of TOS, it is important to differentiate TOS from other conditions presenting with similar symptoms.
TOS imposters include:
Dr. Kalika’s extensive expertise in diagnostic ultrasonography and knowledge of human anatomy equips him to differentiate between TOS and other shoulder conditions. Our advanced ultrasound technology has capabilities for superb microvascular imaging, helping us to detect blood flow restrictions originating in the neurovascular bundle.

Scapular dyskinesis – abnormal movement of the scapula during shoulder motion – can be a contributing factor in TOS. Scapular dyskinesis often involves forward head posture and rounded shoulders due to weak or dysfunctional shoulder stabilizers, altering scapular positioning, which can narrow the thoracic outlet.
Dynamic scapular stabilization requires well-coordinated muscle activation patterns, especially of the rotator, deltoid, trapezius and rhomboid muscles. ShowMotion is an objective tool for joint movement analysis that uses motion tracking sensors, placed on the patient’s skin to collect data about movement quality. Combining scapular ultrasound with ShowMotion technology provides valuable information for diagnosing and treating thoracic outlet syndrome.

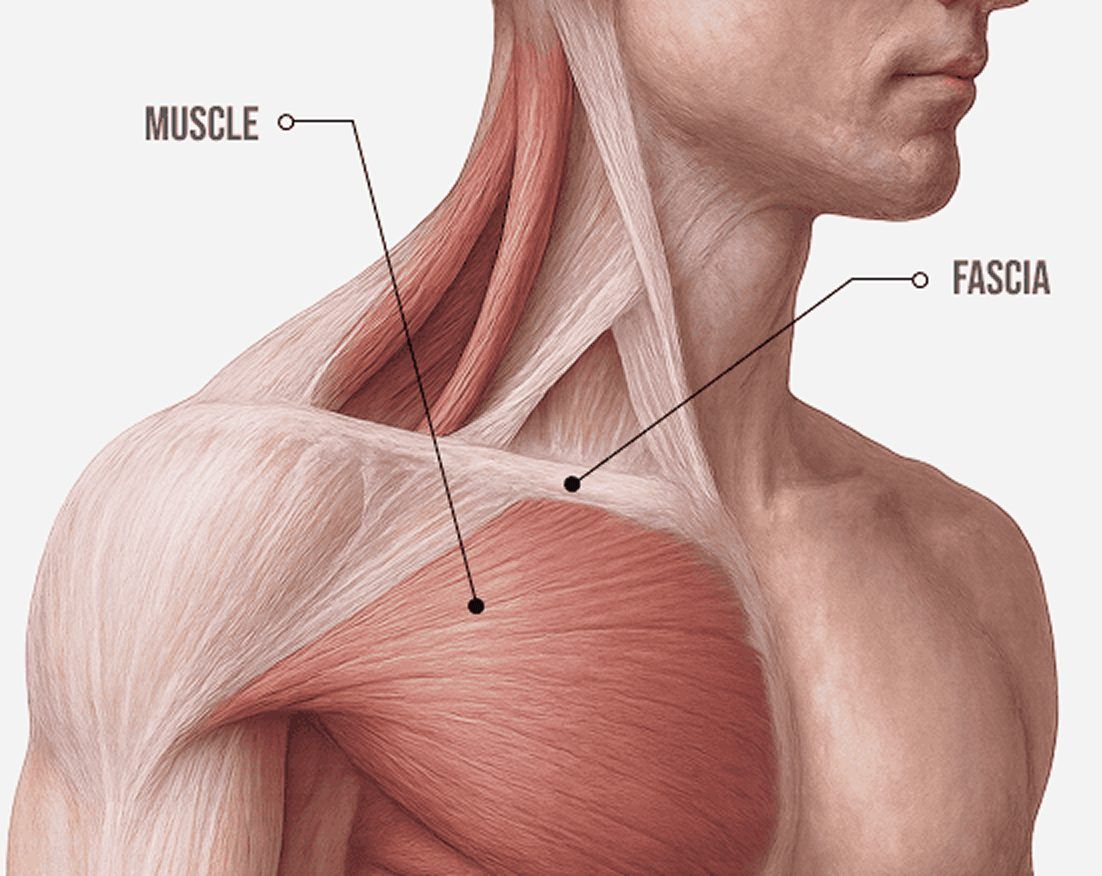
Fascia is a body-wide network of connective tissue that surrounds and connects muscles, nerves, blood vessels and organs. Fascia plays a significant role in thoracic outlet syndrome (TOS). It works together with muscles to provide elastic tension – biotensegrity – that holds tissues, structures and organs in place during movement while allowing for frictionless gliding of nerves and blood vessels.
Fascia can become tight or restricted due to poor posture, repetitive movements, trauma, or scar tissue from injury or surgery. Tight fascia around the scalene and pectoralis muscles can compress the neurovascular bundle, contributing to TOS. At the same time, myofascial trigger points – hard nodules of tightly contracted fibers – can cause pain and interfere with muscle action, and fascial adhesions can restrict mobility. Identifying and treating fascial dysfunction should be a key component of TOC treatment.

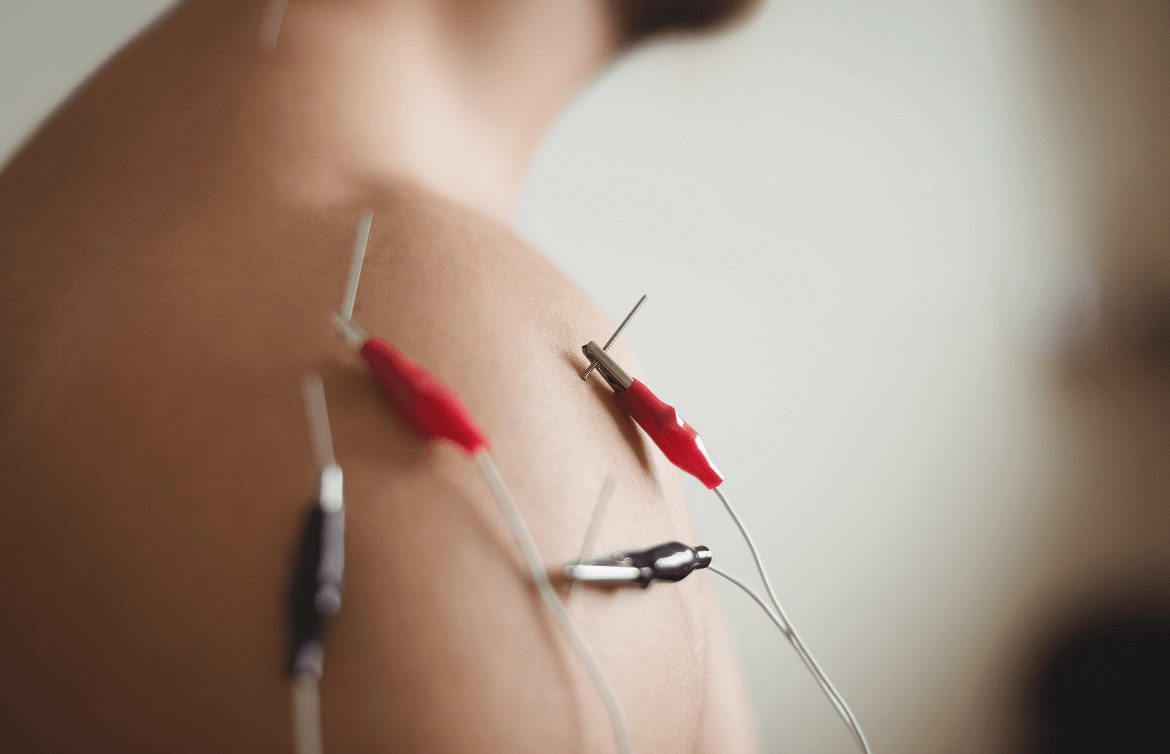
Regenerative therapies are non-invasive interventions that harness the power of sound, electromagnetic, and radiofrequency waves to stimulate a healing response in damaged tissues. The waves promote healing by attracting stem cells, growth factors and other biological agents to the treatment site. We use regenerative technologies in conjunction with manual therapies, orthobiologics, and physical therapy to enhance treatment effects and accelerate recovery from TOS syndrome.




Orthobiologic injection therapies use natural/neutral solutions, injected with precision thanks to ultrasound guidance. The injected solutions stimulate cellular repair by either nourishing or irritating the targeted cells. Orthobiologics are also effective for separating densified fascial layers and restoring their functional properties. Ultrasound guidance ensures injection accuracy and protects nerves and blood vessels from accidental penetration.




For non-athletes, one of the key contributors to TOS is being out of shape. When the muscles that support your upper body are weak, tight or imbalanced, the structures can collapse on themselves, leading to nerve compression, vascular restriction, joint misalignment and reduced range of motion. A resistance training program designed to balance muscle tension and optimize posture can dramatically reduce your risk of developing TOS.
For athletes, ample recovery time between training sessions is essential. Massage, stretching and cross-training exercises can help to balance muscle tension and prevent the thoracic outlet from narrowing. Cold therapy can help reduce inflammation that contributes to TOS.

The neck and shoulder region is made up of a complex network of bones, muscles, connective tissues, nerves, and blood vessels, and many factors can contribute to thoracic outlet syndrome. At NYDNRehab, we use high-resolution ultrasound imaging to differentiate TOC from imposters. Our holistic and personalized approach ensures that you get the most appropriate TOS treatment, for fast and enduring results, without drugs or surgery.





Conference Abstract
2019
 Lev Kalika
Lev Kalika  Rostyslav Bubnov
Rostyslav Bubnov Conference Abstract
2020
Lev Kalika Rostyslav Bubnov Conference Abstract
October 2025
 Lev Kalika Rostyslav Bubnov
Lev Kalika Rostyslav Bubnov Conference Poster
September 2025
Lev Kalika Rostyslav Bubnov 
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination