March 6, 2025

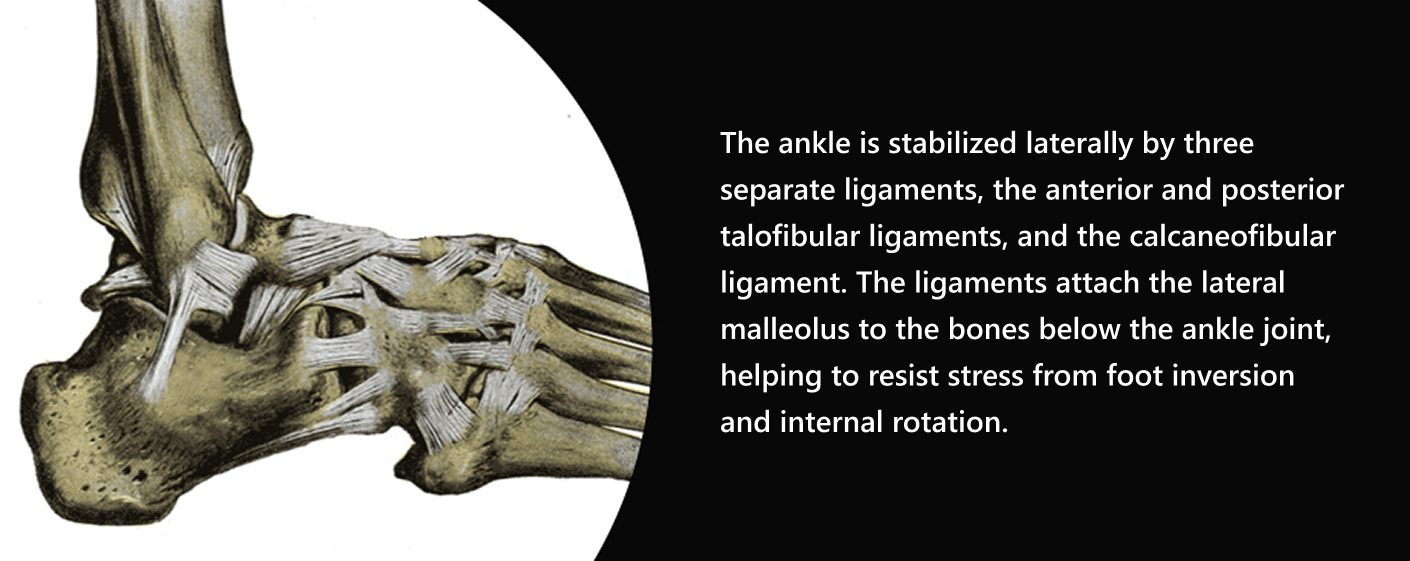
The ankle is a hinged synovial joint that works in concert with the subtalar joints to plantar flex and dorsiflex the foot. Tough ligaments made of Type 1 collagen are the primary stabilizing structures of the ankle, while musculotendinous tissues work to produce, absorb and control forces. The ankle is stabilized laterally by three separate ligaments, the anterior and posterior talofibular ligaments, and the calcaneofibular ligament. The ligaments attach the lateral malleolus to the bones below the ankle joint, helping to resist stress from foot inversion and internal rotation.
The structures of the ankle are highly adaptable to the specific types of demands placed on them. For example, a hockey player’s ankles adapt to training differently than a basketball player’s ankles. Strengthening exercises that specifically target the feet and ankles can help prevent sprains and preserve ankle stability.
When an ankle becomes unstable, it can affect muscle activation patterns along the entire kinetic chain, in both the injured and non-injured sides of the body. One recent study used surface EMG (SEMG) to compare muscle activation in participants with unilateral chronic ankle instability (CAI) and an uninjured control group. They monitored the participants on a split-belt treadmill, with and without random left- and right-sided perturbations.
Research results found that:
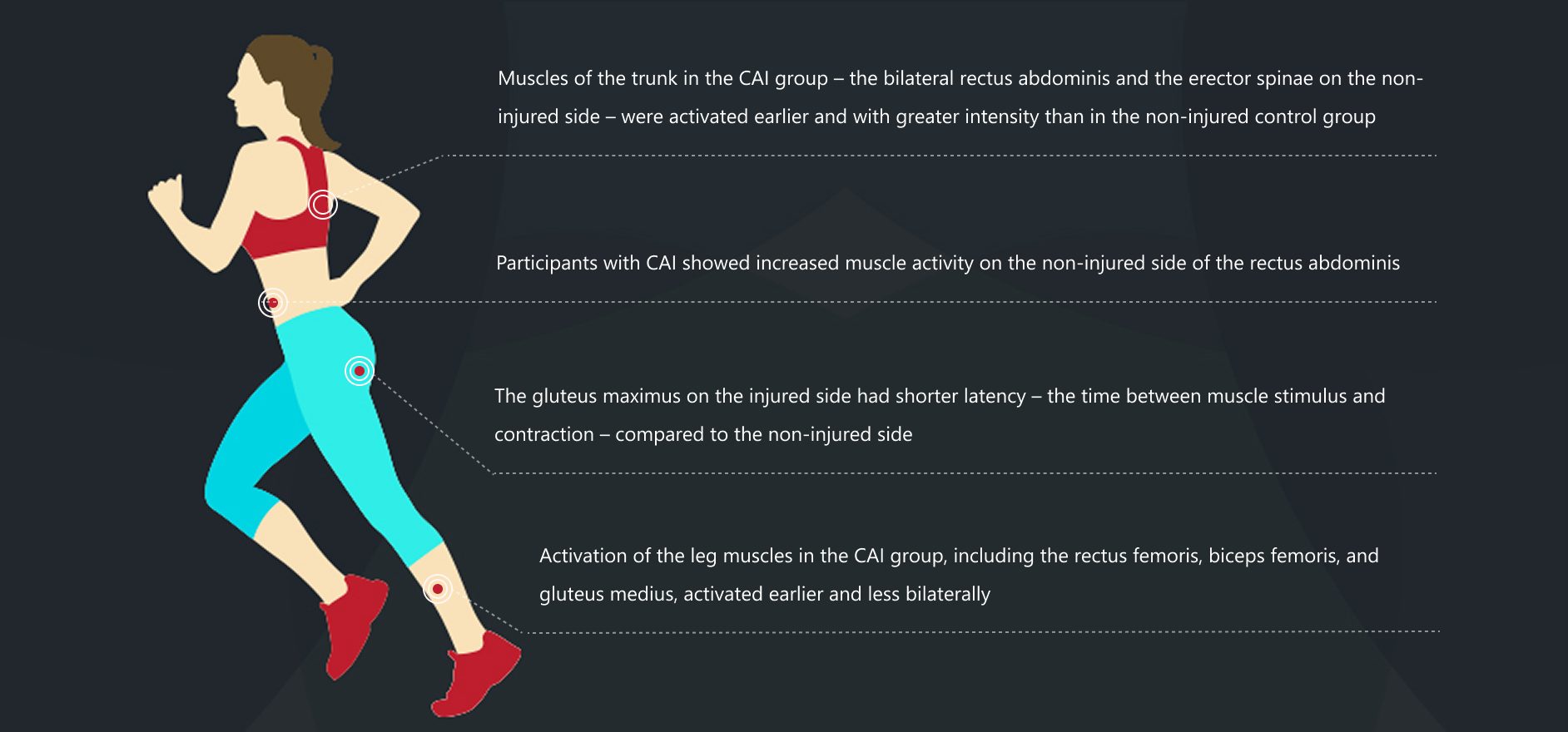
The research team concluded that unilateral CAI alters bilateral motor control strategies around proximal joints. Altered muscle activation patterns reduce movement efficiency, increase injury risk and lower physical performance. Over time, unilateral CAI can cause postural issues that contribute to joint pain and other issues.
In physically active and athletic populations, chronic ankle instability often manifests after a lateral ankle sprain, a common injury that involves the foot and ankle rolling inward at a high velocity during sports or exercise. Lateral ankle sprains account for about 30% of all injuries, with a 73% chance of re-injury. Of those injured, as many as 40% will develop CAI.
Symptoms of CAI include:





Injury to the ankle ligaments can cause damage to the proprioceptors that signal the central nervous system to influence neuromuscular control, not only of the ankle joint, but also control of the proximal joints.
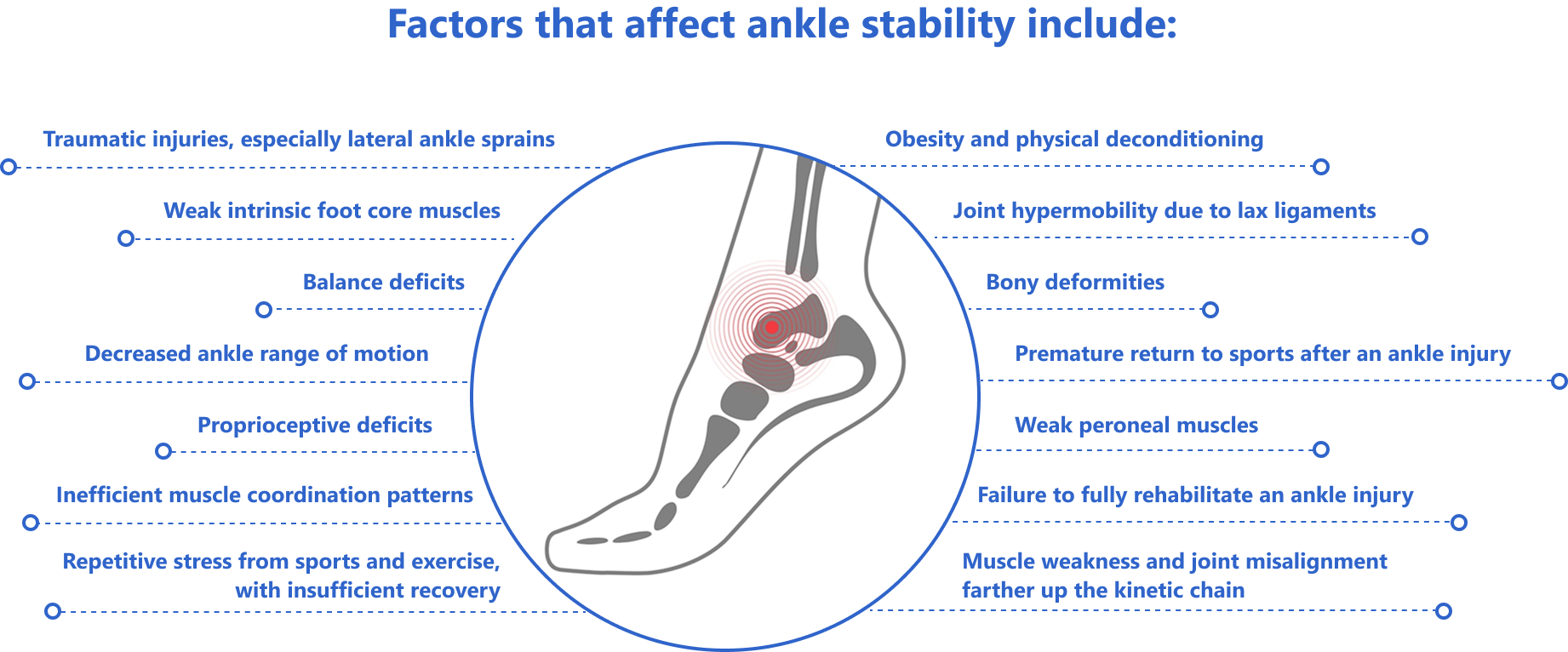
Factors that affect ankle stability include:
CAI rehabilitation is geared toward muscle strengthening, range-of-motion exercises, regenerative therapy to repair and rearrange joint cartilage, neuromuscular feedback training, postural realignment, and eradication of compensation patterns.
There are a number of clinical tests for CAI, some of which require the patient to jump and land. But in the early stages of ankle injury, patients are often incapable of jumping, and attempting to land on an injured ankle can make things worse. Thankfully, new technologies are changing the game for CAI assessment.

Advanced diagnostic ultrasound imaging takes the guesswork out of ankle instability assessment, providing a window into the structures that affect ankle function. Ultrasound is useful for comparing the injured and uninjured ankles, visualizing how the ankle structures interact, identifying facial densification and myofascial trigger points, and guiding therapeutic procedures. Capabilities for Superb Microvascular Imaging (SMI) and sonoelastography provide invaluable tools for monitoring the rehabilitation process.
2. Star Excursion Balance Test
The Star Excursion Balance Test (SEBT) is a dynamic test that measures strength, flexibility, and proprioception. It is widely used to measure dynamic postural control, and it is extensively used to test for chronic ankle instability. NYDNRehab has customized the SEBT for 3D motion analysis.
A high-tech gait analysis using sophisticated equipment and customized software can reveal quantitative details about ankle instability, and its effects on functional performance. When combined with a wearable dynamic ultrasound device, 3D running gait analysis provides data on functional performance that can be used for rehabilitation and athletic performance enhancement.
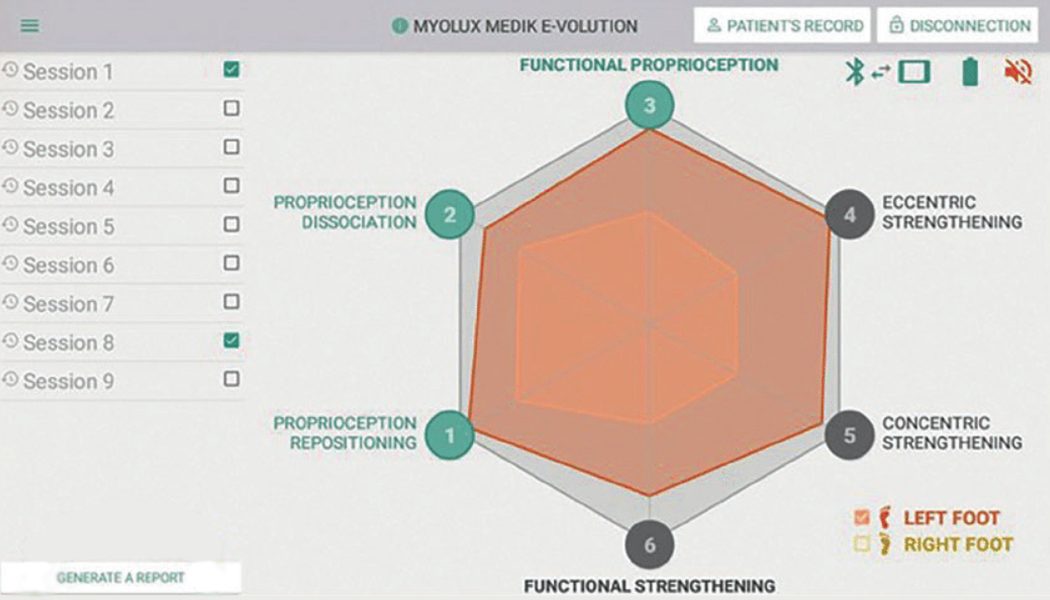
The Myolux system was developed in France to assess and rehabilitate foot and ankle functional deficits. MyoLux is used to test and assess ankle proprioception. Its envelope of function measures the upper and lower thresholds of load that the ankle can tolerate. Myolux also serves as a re-education device to promote and restore ankle stability.
ROAST is a clinical assessment for mechanical and sensorimotor impairments in acute ankle sprains. ROAST is used to establish the mechanism of injury, assess ligaments and bones, and screen for previous ankle injuries. ROAST helps clinicians to identify the risk of developing CAI in the early stages of injury.
Because ligaments have limited vascularity, it was previously thought that once a ligament had been stretched and torn, surgery was the only hope for restoring ankle stability. But new technologies and advancements in research are debunking that notion, offering alternative approaches to treating CAI.
Tissues like ligaments and tendons have less blood flow – and hence receive less oxygen and fewer nutrients – so they heal more slowly than other soft tissues. The ankle tendons are supplied with blood by the anterior tibial, posterior tibial, and peroneal arteries, and respond well to regenerative interventions. Although severe cases may require surgery, most ankle instability can be successfully treated conservatively.
Treatment options for CAI include:
There are a number of things you can do to minimize your risk of developing CAI:

Ankle instability can dramatically affect your performance and increase your risk of injury, both now and in the future. As you age, chronic ankle instability can increase your risk of falls and contribute to joint and muscle pain. Early treatment after an ankle injury and full-spectrum rehabilitation are your best bets for enjoying a lifetime of physical activity and functional pain-free movement.
To get the most advanced and comprehensive CAI treatment in NYC, contact NYDNRehab today!
Ahern, Leanne, et al. “Effect of functional rehabilitation on performance of the star excursion balance test among recreational athletes with chronic ankle instability: a systematic review.” Archives of rehabilitation research and clinical translation 3.3 (2021): 100133.
https://www.sciencedirect.com/science/article/pii/S2590109521000379
Kim, Jin-Hong, Dong-Jin Lee, and Eun-Sang Lee. “Effects of Intrinsic Foot Muscle Exercise on Dynamic Balance, Strength, and Vibration Threshold Sense in Persons with Ankle Instability.” PNF and Movement 18.2 (2020): 173-182.
https://koreascience.kr/article/JAKO202029565213847.pdf
Lin, Chiao-I., et al. “The effect of chronic ankle instability on muscle activations in lower extremities.” Plos one 16.2 (2021): e0247581.
The effect of chronic ankle instability on muscle activations in lower extremities
Tedeschi, Roberto, et al. “Rebuilding Stability: Exploring the Best Rehabilitation Methods for Chronic Ankle Instability.” Sports 12.10 (2024): 282.
https://www.mdpi.com/2075-4663/12/10/282
Werasirirat, Phurichaya, et al. “Effect of supervised rehabilitation combined with blood flow restriction training in athletes with chronic ankle instability: a randomized placebo-controlled trial.” Journal of exercise rehabilitation18.2 (2022): 123-132.
https://www.e-jer.org/journal/view.php?number=2013600933

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































