May 22, 2024
Lower back pain (LBP) is one of the most common musculoskeletal complaints worldwide, affecting more than 600 million adults, according to the World Health Organization (WHO). Within that demographic, the National Institutes of Health (NIH) estimates that only 5-10% of patients with low back pain actually have sciatica. Despite those statistics, medical doctors are quick to diagnose sciatica as the primary cause of LBP when in fact there are multiple other conditions that share similar symptoms.
Learn about true sciatica, the imposters that imitate it, and how high resolution diagnostic ultrasonography can help to differentiate between the various causes of sciatica-like pain symptoms.
True sciatica arises when the sciatic nerve – the longest and widest nerve in the body – is compressed or impinged by a herniated disc or by osteoarthritic bone spurs at one of its roots in the lower spine. But the sciatic nerve travels a long path beyond its nerve roots, innervating the lower extremities all the way to your feet.
The sciatic nerve can potentially become compressed, entrapped or irritated by structures and tissues anywhere from your pelvis to your distal thigh, creating symptoms of false sciatica. When that happens, treating the area surrounding the nerve root is unlikely to provide relief.
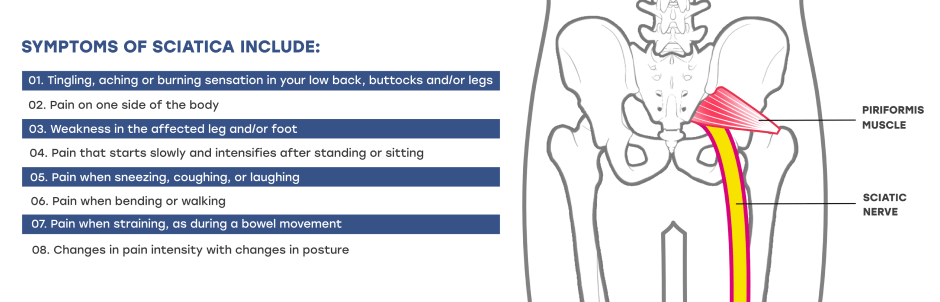 Symptoms of sciatica include:
Symptoms of sciatica include:There are multiple extra-spinal conditions that mimic sciatica symptoms. Because sciatica is most often diagnosed based on symptoms and a physical exam, doctors can easily overlook other conditions with similar symptoms that can be mistaken for sciatica.
Sciatica diagnosis based on symptoms is a hit-or-miss approach, where doctors wait to see if the prescribed treatment works before considering whether the patient’s pain is caused by sciatica or something else. This inefficient diagnostic approach can prolong the patient’s suffering and create unnecessary financial challenges.
When sciatica-like pain does not respond to treatment, MRI may be recommended to visualize the affected area. However, a regular MRI gives us static images that do not shed much light on the underlying pathology. Only an MRI neurography is capable of providing useful images of nerve entrapment, and that can cost between $8000-12,000, which is rarely covered by insurance.

Although MRI can be useful for larger patients due to its depth of penetration, ultrasonography has multiple advantages over MRI. High-resolution ultrasound provides detailed images of nerve compressions as they happen, along with other factors that affect the subgluteal space, without exposing the patient to radiation or toxic heavy metals. Patient discomfort is minimal, and results are instantaneous, expediting appropriate treatment.

Advantages of ultrasound imaging include:
Sciatic nerve pain is not a medical condition in itself, but a symptom created by other factors. Accurate diagnosis is key in selecting the most appropriate and effective treatment approaches. In most cases, sciatic nerve treatment requires a multifaceted approach, depending on the location of entrapment and the unique characteristics of the individual patient.

In certain stubborn cases, ultrasound-guided injections of a local anesthetic and/or cortisone can sometimes facilitate rehabilitation by numbing pain and reducing inflammation, making it possible to proceed with physical therapy.
An inaccurate diagnosis of sciatica-like symptoms can prolong your pain and discomfort while costing you thousands in medical bills without resolving your condition. At NYDNRehab, we use advanced diagnostic tools to accurately identify your condition. Our personalized treatment approach is based on your unique anatomical characteristics. Our expertise coupled with a broad array of advanced treatment options ensures that your condition is quickly and effectively resolved.
To get the most accurate diagnosis and effective treatment for your low back pain and sciatica-like symptoms, contact NYDNRehab today.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































