July 30, 2024
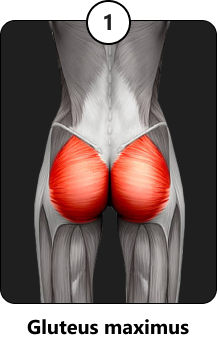
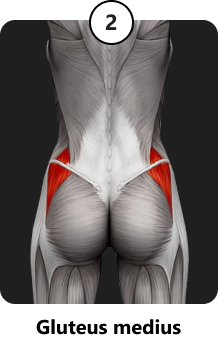
 Your buttocks are made up of a group of four powerful muscles – the gluteus maximus, gluteus medius, gluteus minimus and tensor fascia lata. They work together to extend, rotate, abduct and adduct the hip. Their location in the lumbopelvic region means your buttocks share space with multiple organs, nerves, blood vessels and bony structures. Buttocks pain can arise from a variety of causes, so it’s critical to get an accurate diagnosis before initiating treatment.
Your buttocks are made up of a group of four powerful muscles – the gluteus maximus, gluteus medius, gluteus minimus and tensor fascia lata. They work together to extend, rotate, abduct and adduct the hip. Their location in the lumbopelvic region means your buttocks share space with multiple organs, nerves, blood vessels and bony structures. Buttocks pain can arise from a variety of causes, so it’s critical to get an accurate diagnosis before initiating treatment.
Learn about the various potential causes of buttocks pain, the most sophisticated diagnostic tools for differentiating among them, and the most advanced evidence-based treatment options.
The muscles of the buttocks and lower back provide hip and pelvic stability, enabling humans to stand erect and walk upright. They work with the abdominal muscles to mediate force loads between the upper and lower body, providing dynamic stability during physical activity. Weakness and imbalances in gluteal muscle tension can cause a broad range of mechanical issues that impact other structures within the pelvis and along the lower kinetic chain.
Major muscles of the buttocks are:


A group of smaller muscles called the deep lateral rotators work with the gluteals to laterally rotate the leg. They Include the quadratus femoris, piriformis, gemellus superior, gemellus inferior and obturator internus.
Because your buttocks span the posterior pelvis, they interact with numerous nerves and blood vessels that supply the lower extremities. The buttocks can profoundly affect other pelvic structures such as the sacroiliac joints that connect the spine to the pelvis.
Modern lifestyles that involve extensive bouts of sitting can cause the buttocks to weaken and become lax, impeding their function as stabilizers. Sitting also weakens the abdominals. Weak abs and glutes dramatically reduce your ability to mediate forces, increasing your risk of back and buttocks pain.
The complex architecture of the pelvic region encompasses multiple organs and structures, including the lumbosacral spine, sacroiliac (SI) joints, hip joints, and numerous nerves and blood vessels. Multiple muscles and a network of fascia provide tensile integrity – tensegrity – to guide and control movement and hold the various structures in place.
Buttocks pain is a symptom that can arise from a variety of causes, and treating the locus of pain is unlikely to resolve it. A skilled practitioner with an in-depth knowledge of pelvic anatomy, along with expertise in high-resolution ultrasound imaging, are needed to accurately diagnose buttocks pain. Unlike MRI, diagnostic ultrasonography enables dynamic visualization of the pelvic structures in real time.

High resolution imaging allows clinicians to:
A clinical diagnosis made without dynamic high-resolution ultrasonography is essentially a guessing game, turning the patient’s condition into an experimental testing ground for a broad range of treatments and drugs. Without an accurate diagnosis, patients can suffer for months or even years while draining their bank accounts in hopes of resolving their condition.
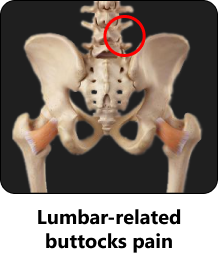
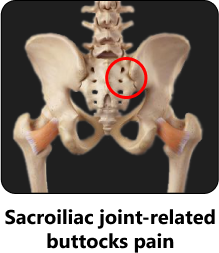
There are four general subcategories of buttocks pain: lumbar-related, SIJ-related, hip joint-related and myofascial-related. Pain may arise from a single cause, or from a combination of factors.
Buttocks pain originating from the lumbar spine is most often related to nerve compression, either from stenosis, disc herniation, or facet joints. It often involves compression of the sciatic nerve somewhere along its path, often causing buttocks pain where it runs beneath the piriformis muscle.
Lumbar-related characteristics are:
SIJ-related buttocks pain is grossly over-diagnosed, and efforts to reposition the pelvis and enhance pelvic stability can sometimes do more harm than good. Patients are often convinced that they need frequent adjustments to realign the pelvis, when in fact the SI joint may not be the source of pain. SIJ-related buttocks pain is most common in pregnant and postpartum patients, and in patients who have suffered pelvic trauma.
Characteristics of SIJ-related buttocks pain are:

Hip-related causes of buttocks pain are commonly overlooked, leading to maltreatment or undertreatment of the condition. Posterior femoroacetabular impingement (FAI) and chondrolabral pathology are conditions affecting the ball-and socket architecture of the hip, where the head of the femur rubs against its socket, creating friction that can tear the labrum – the socket lining – and damage the hip’s articular cartilage. FAI often affects patients with joint hypermobility syndrome. Hip-related buttocks pain can also be linked to hip osteoarthritis.
Characteristics of hip-related buttocks pain are:
Myofascial pain syndrome is a common cause of buttocks pain affecting the large gluteus maximus and gluteus medius muscles. Myofascial pain can be generated from entrapment of the sciatic nerve, the posterior femoral cutaneous nerve, or the superior gluteal nerve. Pain can also be generated by myofascial trigger points – tightly contracted knots of muscle fibers that cause a sharp pain in the buttocks when pressed.
Myofascial buttocks pain symptoms include:
Other sources of buttocks pain that do not fall under the above categories include:
Once the exact source of your buttocks pain has been identified and confirmed, there are a plethora of therapeutic approaches available, including regenerative technologies, injection therapies and specialized physical therapy.
Prior to beginning physical therapy, you may need to resolve issues such as:
Your clinician may use regenerative technologies and orthobiologic injections to repair tissues, reduce inflammation, address myofascial issues, and release entrapped nerves.
Focused ESWT is an evidence-based approach to treating damaged tendon, muscle and bone tissue. This technology produces high frequency sound waves to stimulate the body’s own reparative mechanisms. It is especially effective for chronic degenerative tendon disorders and myofascial pain syndrome.
MyACT is a new type of focused shockwave technology whose higher frequency allows for precise neuro modulation under ultrasound guidance, with a special linear head for treating myofascial pain. MyACT transforms the mechanical energy of shockwaves into biochemical signals that precisely target damaged tissues, to stimulate the body’s own reparative mechanisms.
EMTT transmits high energy magnetic pulses to targeted tissues that synchronize with the body’s own magnetic fields, triggering a regenerative response. EMTT waves can penetrate deep tissues to target difficult-to-reach tendons, muscles, bones and nerves.



Transcutaneous magnetic neuromodulation delivers high-intensity magnetic pulses to peripheral tissues, to stimulate neuroplasticity. This FDA-approved methodology is used to treat pain and regenerate nerve fibers, for enhanced motor control.
Neuralign S is a therapeutic Motion Activated Stimulation technology that uses advanced sensors coupled with neuromuscular electrical stimulation. This breakthrough technology helps patients to recalibrate muscle actions, to optimize joint function. Neuralign S is revolutionizing the way shoulder injuries and rotator cuff tears are treated and rehabilitated.

The Stecco method of fascial manipulation involves deep friction that heats up tissues and stimulates mechanical action. Stecco fascial manipulation is an evidence-based methodology for treating densified fascia, and breaking up scar tissue and adhesions. Stecco therapy is often used in conjunction with regenerative technologies. Patients often report immediate pain relief after a single Stecco session.
Injection therapies use natural or neutral solutions to stimulate cellular repair by either nourishing or irritating the targeted cells. It is important to note that injection therapies are most effective when guided by high-resolution ultrasonography, to ensure that the needles precisely hit their target.
PRP therapy uses a centrifuge to extract a high concentration of platelets from a sample of the patient’s own whole blood. When injected into damaged tissues, PRP releases biologically active factors to initiate the synthesis of new connective tissues and blood vessels.
Prolotherapy uses a biologically neutral solution to irritate stubborn tissues, triggering a regenerative response to grow new normal tendon, ligament and muscle fibers.
Buttocks pain often stems from densified fascial tissues that have formed adhesions, entrapping nerves and blood vessels. Hydrodissection injects a saline solution into densified fascia to separate fascial layers and free up entrapped nerves and blood vessels. Hydrodissection is often used in conjunction with manual fascial manipulation.
Dry needling targets myofascial trigger points by inserting thin non-medicated needles to evoke a twitch response, relaxing contracted fibers and immediately relieving pain.
At NYDNRehab, we begin your therapy journey with high-resolution diagnostic ultrasonography, to get a clear picture of your condition. Once we identify the source of your buttocks pain, we pretreat your tissues to protect them from further injury. Only then will you be ready for specialized buttocks pain physical therapy.
Dr. Lev Kalika is an expert in diagnostic musculoskeletal ultrasonography and shockwave therapy. He has published multiple scientific papers on ultrasound guided procedures, and his research is frequently presented at medical conferences such as the International Society for Medical Shockwave (ISMS) Congress.
The clinic at NYDNRehab features an impressive array of technologies, including the most advanced high-resolution ultrasound equipment. We are one of the few clinics in Manhattan to offer regenerative therapies, orthobiologic injections, and personalized one-on-one physical therapy.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































