March 12, 2025

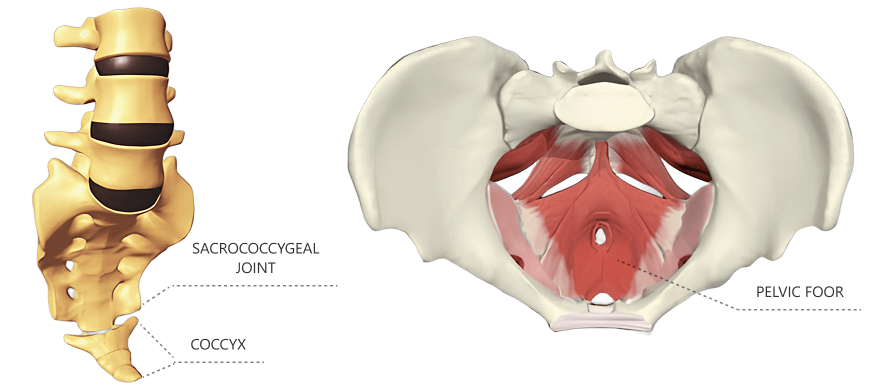
The coccyx – aka tailbone – is the bony segment at the very end of the spinal column, right below the sacrococcygeal joint, consisting of 3-5 segments. Coccydynia refers to pain in the coccygeal bone and/or its surrounding tissues. In most cases, tailbone pain has an acute onset due to traumatic injury, and most cases self-resolve over a matter of weeks. However, tailbone pain that lasts longer than two months is defined as chronic coccydynia, marked by a consistent nagging pain that makes sitting uncomfortable.
Learn about the causes of coccydynia, the populations most often affected by it, and advanced therapeutic approaches that successfully resolve chronic coccydynia.
Tailbone pain arises from the coccygeal plexus – a network of nerves that originates in the lower sacral spinal cord. The nerves carry sensory information and transmit pain signals from the tailbone area to the brain. Coccydynia occurs most often in females of all ages, although it may also arise in men. In most cases the condition is considered mild, and it typically self-resolves in a matter of weeks as the injured tissues heal.
Common causes of coccydynia include:









Persistent tailbone pain lasting two months or longer can be conservatively managed by treating pain symptoms, resulting in spontaneous improvement in about 90% of patients. In the remaining 10 percent of cases, chronic coccydynia can diminish your quality of life, interfering with everyday activities and making it painful to move and sit down.
People with chronic coccydynia may experience pain during intercourse, and some report difficulty defecating. You may experience sharp pain when rising from sitting to standing, and sitting on hard surfaces may be unbearable. When provided by an experienced practitioner, specialized coccydynia physical therapy can help resolve chronic tailbone pain and restore pain-free functional movement.
Treatment options range from sitting on a special cushion to full-blown coccygectomy – a surgical procedure to completely remove the coccyx. If coccygeal pain originates from the pelvic floor, specialized pelvic physical therapy can help to resolve the condition.
To determine the most effective treatment options, one research team conducted a broad systematic review of the various treatment modalities for coccydynia.
Research results revealed:

The researchers recommended non-invasive treatments like radiofrequency therapy and shockwave therapy for tailbone pain, over riskier, more invasive and irreversible coccygectomy.
The team at NYDNRehab has an impressive track record of resolving over 500 cases of coccydynia. Our clinic features the most advanced technologies available for diagnosing and treating a broad spectrum of musculoskeletal conditions and injuries. We conduct a comprehensive exam on your first visit using high-resolution diagnostic ultrasonography, to confirm the exact cause of your tailbone pain and rule out other causative factors.
NYDNRehab is one of only a few private clinics to offer INDIBA radiofrequency therapy, along with a broad range of shockwave technologies, including SoftWave, MyAct, focal and radial shockwaves. Tailbone pain often affects more than one tissue type, and requires a combination of different shockwaves to completely eliminate pain.
Our expertise, technologies, holistic approach, and track record of success make NYDNRehab the clinic of choice for coccydynia physical therapy in MIdtown Manhattan.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































