Patellofemoral pain syndrome (PFPS), also known as runner’s knee or jumper’s knee, is a common condition among runners and athletes. PFPS is a generalized term used to describe pain at the front of the knee and around the patella (kneecap). The condition is especially prevalent in young female athletes, but it can affect anyone, at any age, including non-athletic populations of both sexes.
or
Clinical director & DC RMSK
Verified Expert Profiles
Dr.Kalika has revolutionized knee pain treatment by introducing high resolution diagnostic ultrasonography for structural diagnosis, combined with gait and motion analysis technology to visualize and objectify the functional movement of the lower extremities.
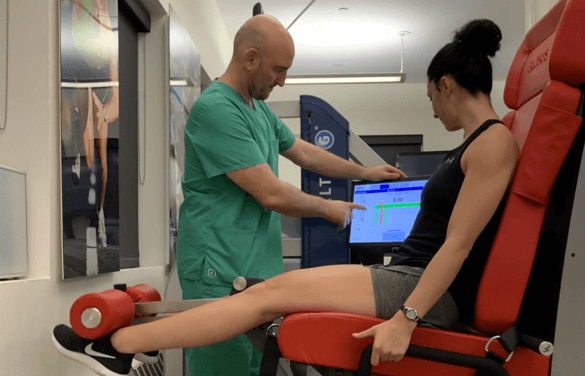
The motion and gait analysis lab at NYDNRehab is the only private lab in the US to feature research-grade technology, normally found only at top research universities, and made available to patients in our private clinic. Dr.Kalika believes that what cannot be measured cannot be treated. We fully analyze and quantify joint angles, ground reaction forces, muscle firing patterns, weight distribution and more, to get to the bottom of your knee pain and correct it.
Dr.Kalika’s expertise is sought by professional athletes, runners and dancers across the United States.
Many conventional physical therapists take a one-size-fits-all approach to patient care, using antiquated timelines and cookie cutter exercises that fail to fully rehabilitate knee injuries and restore optimal movement.
At NYDNRehab, we take an individualized approach to every patient and every condition. Using advanced technologies, we are able to accurately diagnose and measure individual parameters for joint angles, force loads, muscle firing patterns and gait. We then design personalized treatment programs based on collected data, measuring progress along the way to ensure full recovery.
Our experience combining innovative treatment methods with advanced technologies makes NYDNRehab the number one choice for physical therapy, chiropractic care and rehabilitation in NYC.
We use FDA approved methodologies to successfully treat a broad range of conditions. Our patients include elite athletes, runners and ballet dancers who come to us for rehab and performance enhancement.

Pain at the front of the knee and around the kneecap
Pain while squatting or climbing stairs
Pain after long periods of sitting with bent knees
Crackling or popping sounds or sensations in your knee
Pain that increases with changes in activity or playing surface
Repetitive overuse from sports and exercise
Kneecap misalignment
Weak or imbalanced muscles
Improper biomechanics
Unsupportive footwear and hard playing surfaces
Participation in running, cutting and jumping sports
Young female athletes
Excessive sitting
Overweight or obesity
Changes in intensity and playing surface
The sports medicine specialists at NYDNRehab are experts in diagnostic musculoskeletal ultrasonography. Diagnostic ultrasound not only enables the doctor to identify the structural causes of knee pain, but it allows your clinician to view the knee region in real time, with the knee in motion. In addition, 3D gait analysis helps us to identify faulty movement mechanics that contribute to PFPS pain.
By visualizing the knee in motion and gathering quantitative data about gait mechanics, we are able to establish a baseline against which to measure progress. Once the exact cause of PFPS pain is determined, an effective treatment plan can be initiated and objectively measured for effectiveness.
PFPS pain can range from mild to excruciating, and chronic PFPS is often treated with pain medications and steroid injections. However, most non-traumatic knee pain can be eliminated through the non-invasive treatment methods we practice at NYDNRehab. We use the latest technologies and innovative therapies to treat PFPS at its source and eliminate it for good.
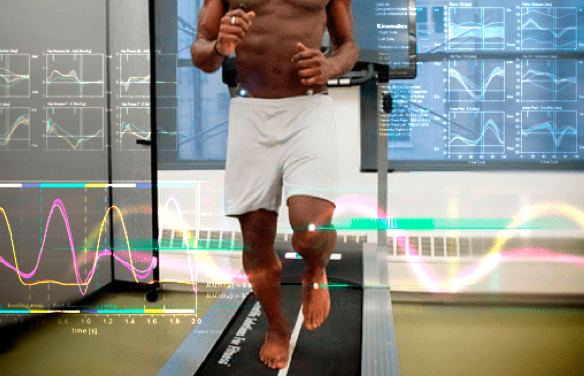
Mechanical deficiencies in walking or running gait can cause the knee to become misaligned, placing undue stress on the structures surrounding the knee and producing pain. We use our state-of-the art gait lab to analyze joint angles and force loads associated with gait, to identify and quantify mechanical deficits and retrain the way you walk and run, to eliminate pain.

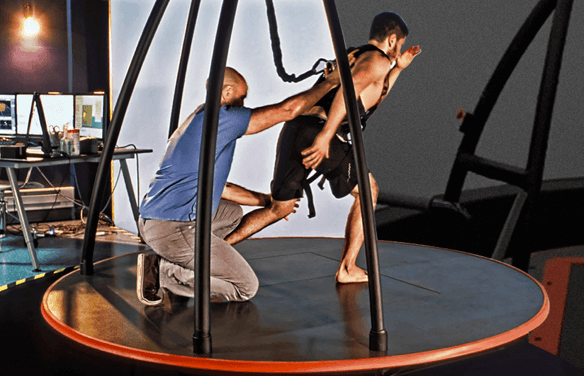
Our gravity-reducing treadmill unloads the knee joint, to enable retraining of gait patterns without placing undue stress on injured structures. This approach speeds recovery by allowing gradual reloading of the knee and gradual improvement of gait patterns.
C.A.R.E.N’s advanced technology uses a virtual reality environment to train healthy movement patterns and enhance sports performance. Real-time feedback is provided to optimize motor patterns, retraining the brain-body connection for efficient pain-free movement.
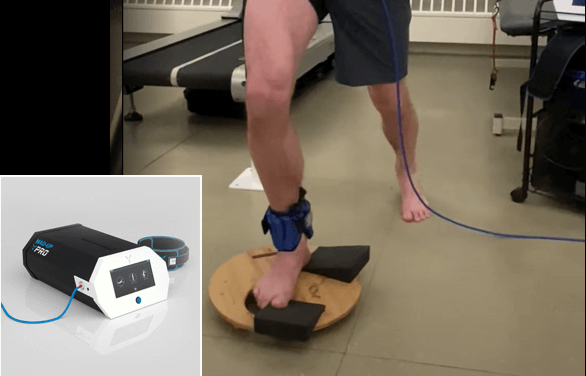
BFR makes it possible to rehabilitate injured tissues using much lighter loads, by occluding the blood vessels to elicit a regenerative response in damaged cells. BFR helps prevent tissue atrophy after an injury while protecting damaged structures from overload. It speeds the recovery process for faster return to pain-free activity.
Physical therapy exercises work to strengthen and rebalance the muscles that support the knee joint, taking pressure off of nerves and connective tissue, and realigning the joint for optimal function.
The human body has its own innate healing mechanisms, but it sometimes needs a nudge to accelerate the healing process. Regenerative technologies help to jump-start healing by stimulating tissue repair at the cellular level. Our outpatient regenerative therapies expedite recovery with minimal discomfort for the patient.
Focused ESWT is used as a regenerative treatment for damaged tendon, muscle and bone tissue. This technology produces high frequency sound waves to stimulate the body’s own reparative mechanisms. It is especially effective for chronic degenerative tendon disorders and myofascial pain syndrome.
EMTT is a fairly new technology that transmits high energy magnetic pulses to targeted tissues. The magnetic waves synchronize with the body’s own magnetic fields, causing a disturbance that triggers a regenerative response. EMTT waves can penetrate deep tissues up to 18 cm beneath the skin’s surface, to target difficult-to-reach tendons, muscles, bones and nerves.

Extracorporeal Pulse Activation Technology (EPAT)
EPAT, also known as defocused shock wave therapy, uses acoustic pressure waves to enhance blood circulation to targeted tissues. This speeds up the delivery of oxygen and nutrients to damaged tissues and stimulates cellular metabolism, to accelerate the healing process.
HEIT uses electromagnetic fields to penetrate cells, tissues, organs and bones, to reactivate the electrochemical function of cells and cell membranes. HEIT generates a magnetic field 600 times stronger than the field of a normal magnet, to stimulate healing of nerves, muscles and blood vessels.

Our INDIBA Tecar therapy machine converts electrical current into a stable radio frequency current of 448 kHz, designed to increase and stabilize the exchange of ions in damaged cells, evoking a regenerative response that accelerates healing. INDIBA can be used to successfully treat joint and muscle disorders, low-back pain, sports injuries, surgical incisions and various pain syndromes. Another therapeutic effect of INDIBA is extreme and prolonged cellular hyperthermia. Due to this effect, INDIBA therapy combined with manual therapy and soft tissue tissue manipulation enables instantaneous release to occur, significantly shortening the number and duration of physical therapy sessions. What is normally accomplished in two months of physical therapy can be accomplished in 3-4 sessions with INDIBA.
Myofascial trigger points often contribute to lower back pain. Dry needling is an outpatient procedure that inserts non-medicated needles into the trigger point to evoke a twitch response, releasing the trigger point and immediately relieving pain. Ultrasound guidance eliminates the need for multiple insertions, reducing pain and discomfort for the patient.

Injection therapies use natural/neutral solutions that stimulate cellular repair by either nourishing or irritating the targeted cells. Guidance by ultrasound ensures that the injected substances hit their mark, for maximum effectiveness.

PRP therapy uses a sample of the patient’s own whole blood, which is spun in a centrifuge to extract a high concentration of platelets. When injected into damaged tissues, PRP initiates tissue repair by releasing biologically active factors such as growth factors, cytokines, lysosomes and adhesion proteins. The injected solution stimulates the synthesis of new connective tissues and blood vessels. PRP can help to jump-start healing in chronic injuries and accelerate repair in acute injuries.
Prolotherapy uses a biologically neutral solution, often containing dextrose, saline or lidocaine. The solution irritates the affected connective tissue, stimulating the body’s own natural healing mechanisms to encourage growth of new normal ligament or tendon fibers.


The best treatment options for acute knee pain depend on the diagnosis. Patellofemoral syndrome is the most common type of acute knee pain.
Treatment options include:
A combination of EPAT (Extracorporeal Pulse Activation Technology) and ESWT (extracorporeal shock wave therapy) to relieve pain and balance tension in the quadriceps muscles and the patellar retinaculum.
Ultrasound guided dry needling
EMTT (electromagnetic transduction therapy) for pain treatment and regenerative therapy
Physical therapy is the single best choice of treatment for chronic PFPS anterior knee pain.


The best way to avoid knee pain and injury is to remain physically active, moving your body in ways that recruit multiple muscle groups in multiple planes of motion. In addition, you should manage your weight and eat a nutrient-dense diet that provides the building blocks for lean muscle and connective tissue. Bone-based broth is a good dietary source of collagen, which plays a protective role in the knee joint.
If you are already physically active, you can benefit from a 3D gait analysis and/or a biomechanical analysis, to identify and correct any motor deficits that can potentially lead to knee injuries. Runners in particular can avoid knee pain by visiting the NYDNRehab Running Lab.
Keeping your hamstring and calf muscles flexible and strong, and your quadriceps strong and balanced will help you avoid knee pain. You should also maintain strong gluteal muscles and a strong core. Do not allow your foot to over-pronate while running, and maintain strong foot core muscles.
It is critical to fully rehabilitate any injuries to the structures of the lower extremity or the low back, including old injuries that were not fully rehabbed.

We understand that every patient has a unique anatomy, and that each condition has unique characteristics. We tailor our one-on-one treatment plans to the individual patient, and never use cookie cutter approaches.
In addition to restoring strength and range of motion to the structures surrounding the knee, we retrain the brain-body connection, to restore optimal neuromuscular recruitment patterns that are often disrupted after an injury. By doing so, our athletes are able to return to sport safely, with reduced risk of re-injury.

Jonas Hoegh-Christensen About NYDNRehab clinic
Jonas Hoegh-Christensen is a famous Danish sailor who has taken part in the Summer Olympics in 2004, 2008 and 2012. He became a men’s sailing champion Finn class in London. Now, Jonas, a holder of an Olympics Silver, is getting ready for the upcoming 2016 Summer Olympics in Brazil. He is thankful to Dr. Kalika that he has managed to resolve all Jonas’s issues quickly and easily. We will cheer for Jonas and hope that this time we will not miss out on the gold.

NY City ballet principal MeganLeCrone testimonial for her returning to dance after hip injury
Watch and hear our patient, ballet dancer Megan LeCrone, explain how her frequent injuries put her in a downward spiral that nearly ended her career. After several surgeries and fruitless therapy, Megan found our clinic and came to us for help. Dr. Kalika was able to help her restore her brain-body connection and build her strength “from the inside-out.” Her pain is gone, her injuries are rehabilitated and she is dancing better than ever. Megan continues to visit the NYDNRehab clinic for maintenance therapy and she feels great! We love our patients, and we never stop until we get to the source of their pain and disability.
If you suffer from chronic knee pain and want to find the best knee doctor in NYC, visit NYDNRehab in midtown Manhattan. Our team of knee pain specialists provide individualized treatment plans to meet the unique needs of every patient. We don’t just treat knee pain – we get to its source and restore healthy pain-free function, so you can enjoy the very best quality of life.
NYDNRehab is the top rated physical therapy clinic for PFPS knee pain in NYC. We accept most health insurance plans, and we are happy to set up payment plans for our patients. Contact us today and make an appointment to get rid of your PFPS knee pain for good, so you can get back to doing the things you love.

Clinical director & DC RMSK
























 Dr. Yuri Brosgol
MD
Dr. Yuri Brosgol
MD
 Dr. Michael Goynatsky
DPT
Dr. Michael Goynatsky
DPT
 Dr. Daniela Escudero
DPT
Dr. Daniela Escudero
DPT
 Dr. Michelle Agyakwah
DC
Dr. Michelle Agyakwah
DC
 Dr. Tatyana Kapustina
L. Ac.
Dr. Tatyana Kapustina
L. Ac.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:Research authored or co-authored by the clinic’s medical director. The following research publications inform the clinical approach used in this treatment program.
Conference Abstract
2024
 Lev Kalika
Lev Kalika  Rostylav Bubnov
Rostylav Bubnov 
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination





















