
Knee meniscus injuries are common among athletes and physically active populations. They also occur in older adults as a consequence of reduced mobility, worn cartilage, and loss of muscle tone. Knee surgeries have become routine for treating meniscus lesions and ruptures, but is meniscus surgery necessary? According to one source, as much as 85 percent of meniscus surgeries are unwarranted, and another source notes that meniscus repair surgeries have a 19 percent overall failure rate.
Learn about the knee meniscus, pros and cons of surgery, and successful alternative therapy for a torn meniscus.
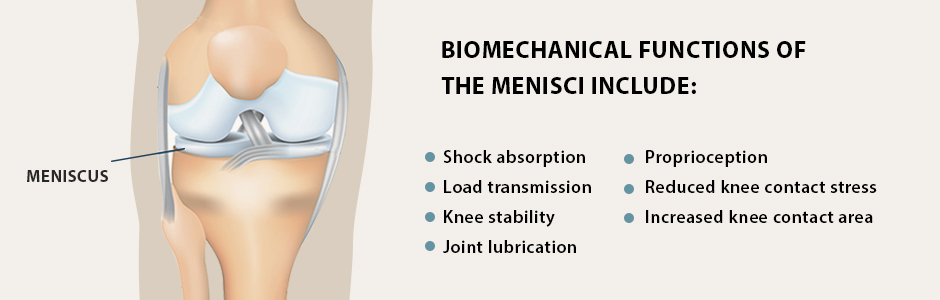
Each of your knees has two menisci — horseshoe-shaped structures of tough fibrocartilage that absorb shock and facilitate smooth gliding of your knee during physical activity. The medial meniscus is located on the inner side of the knee, and the lateral meniscus is on the outer side. The menisci attach to the tibia (shin bone) and provide stability for the knee during load transfer.
Biomechanical functions of the menisci include:
Shock absorption
Load transmission
Knee stability
Joint lubrication
Proprioception
Reduced knee contact stress
Increased knee contact area
Menisci are made up of 65 to 70 percent water, with cross-linked collagen fibers making up about 90 percent of their dry weight. Noncollagenous matrix proteins, such as fibronectin and elastin, make up the remaining 10 percent. Adequate hydration and nutritional support from foods that promote collagen synthesis can help to maintain the health and integrity of the menisci.
Like tendons and ligaments, the menisci are relatively avascular structures, with only a limited peripheral blood supply. When subjected to large force loads, lesions may arise that are slow to heal. Repetitive overload coupled with inadequate recovery time can increase the severity of lesions, resulting in major tears that cause pain and reduce performance. If left untreated, a torn meniscus can set you up for more serious injuries, like an ACL rupture.
Meniscus tissue degeneration in older adults is attributed to “wear and tear” that causes a thinning of meniscal cartilage. Suboptimal hydration, poor nutrition and physical inactivity may be contributing factors. In addition, certain commonly prescribed medications have been found to contribute to chondrocalcinosis, a condition where calcium deposits form in the joints, predisposing the menisci to tears and accelerating the degeneration of meniscus tissue.
The prevalence of asymptomatic medial meniscal tears in adults over age 65 ranges from 30 to 50 percent, increasing incrementally with advanced age. One study of 306 elderly patients aged 65 to 89 years who reported knee pain, with and without knee osteoarthritis (OA), detected lesions of varying degrees in the meniscus of 93 percent of the study participants.
A recent Medicare records study by researchers at Johns Hopkins indicated that surgery to remove damaged meniscus tissue due to degenerative meniscal tears had little to no benefit for patients over age 65. The procedure, called arthroscopic partial meniscectomy (APM), accounts for about two-thirds of orthopedic knee surgeries performed on older adults.
Despite its low value, APM remains one of the most commonly performed surgeries on older adults, with considerable monetary incentives for the medical industry. Meanwhile, new research suggests that conservative care for knee pain in older adults should be the first line of treatment, to completely avoid or significantly delay surgery.
Recommended alternative treatment approaches include:
Physical therapy exercises to strengthen the structures that support the knee
Balance training
Mind-body exercises like tai chi or yoga
Aquatic exercises
Walking
Weight management, to reduce overall load on the knees
In athletes, meniscus tears are very common, often occurring when the athlete pivots on a loaded knee. A tear can also develop over time from repetitive overload, causing the meniscus to gradually lose its resiliency. In some cases, a chunk of the meniscus may even break away, leaving jagged edges behind that cause pain and inflammation.
The traditional treatment of choice for athletic meniscus tears has been meniscectomy, where the damaged portion of the meniscus is surgically removed. However, removal of a portion of the meniscus can have both short and long term negative consequences for athletes.
Decisions about how best to treat a torn meniscus in athletes need to be carefully weighed. Inappropriate treatment can mean missed play time, and can even be career-ending. Treatment of lateral vs medial meniscus injuries must also be taken into account.
Meniscectomies performed on the lateral (outer) meniscus increase contact stresses by 200 to 300 percent, compared to 100 percent in medial procedures. Lateral meniscectomies significantly reduce return-to-play rates, and lateral meniscus tears can be more career-shortening than ACL injuries.
In the short term, medial meniscectomies have a higher return-to-play rate than their lateral counterparts, but athletes who undergo medial procedures are likely to develop medial knee osteoarthritis later on in life.
While there is ongoing controversy about whether surgery is superior to conservative care, the general consensus is that acute traumatic meniscus tears should be treated surgically, followed by physical therapy and rehab, while conservative treatment should be the first line of care for degenerative meniscus lesions.
In addition to exercises aimed at strengthening the knee’s supporting structures, regenerative therapies and injections can stimulate and accelerate the healing of meniscus tears. Regenerative approaches tap into the body’s own innate healing mechanisms, to jump-start and speed up the healing process.
Focused Extracorporeal Shock Wave Therapy (ESWT) is used as a regenerative treatment for damaged tissue. This technology produces high frequency sound waves to stimulate the body’s own reparative mechanisms. It is especially effective for degenerative meniscus conditions.
Extracorporeal Magnetic Transduction Therapy (EMTT) transmits high energy magnetic pulses to meniscus tissues. The magnetic waves synchronize with the body’s own magnetic fields, causing a disturbance that triggers a regenerative response.
When combined, ESWT and EMTT form a dynamic duo that reduce pain and inflammation while speeding up the healing process.
Ultrasound guided injection therapies also trigger a regenerative response in torn meniscus tissue.
Prolotherapy injects a biologically neutral solution to irritate the meniscus tissue, triggering the body’s natural healing mechanisms.
Platelet rich plasma (PRP) therapy injects platelets extracted from the patient’s own blood into the meniscus, releasing biologically active factors such as growth factors, cytokines, lysosomes and adhesion proteins that promote tissue repair.
Surgery of any type has inherent risks. Side effects of drugs and anesthesia, risk of infection, high costs, disappointing outcomes and long-term complications need to be carefully weighed against low-risk alternatives. If you do opt for surgery, you will still need physical therapy for a torn meniscus, to rehabilitate your knee and restore functional movement.
The sports injury specialists at NYDNRehab understand the importance of fully functional knees for athletic populations. We also know how meniscus tears can dramatically impact the quality of life of older adults.
We use high-resolution diagnostic ultrasound to get a clear picture of the type and extent of damage to your meniscus. Our treatment toolbox features the most advanced regenerative therapies and procedures available, to repair and rehabilitate your meniscus injury so you can return to physical activity with confidence.
Resource
Adams, Bryan G., Megan N. Houston, and Kenneth L. Cameron. “The epidemiology of meniscus injury.” Sports medicine and arthroscopy review 29.3 (2021): e24-e33.
Borque, Kyle A., et al. “Evidence-based rationale for treatment of meniscal lesions in athletes.” Knee Surgery, Sports Traumatology, Arthroscopy (2021): 1-9.
Giuffrida, A., et al. “Conservative vs. surgical approach for degenerative meniscal injuries: a systematic review of clinical evidence.” Eur Rev Med Pharmacol Sci 24.6 (2020): 2874-2885.
Reito, Aleksi, Ian A. Harris, and Teemu Karjalainen. “Arthroscopic partial meniscectomy: did it ever work? A narrative review from basic research to proposed disease framework and science of clinical practice.” Acta orthopaedica (2021): 1-10.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































