January 2, 2025
 The human body is uniquely designed to walk on two legs, and walking is our primary form of locomotion. In fact, when you walk, every joint in your body is activated, making walking an ideal form of exercise for anyone. But when you suffer from chronic low back pain, every step can be a challenge, sending pain signals along your central nervous system to your brain.
The human body is uniquely designed to walk on two legs, and walking is our primary form of locomotion. In fact, when you walk, every joint in your body is activated, making walking an ideal form of exercise for anyone. But when you suffer from chronic low back pain, every step can be a challenge, sending pain signals along your central nervous system to your brain.
Many people subconsciously compensate for back pain by altering their gait to reduce force loads on the structures and nerves that cause the most pain. While this strategy may work in the short run, it can become a vicious cycle over time, creating gait abnormalities that cause more back pain.
Learn about gait fundamentals, the connection between low back pain and walking gait, and the benefits of 3D gait analysis.
Due to the shoulder’s multiplanar range of motion, the glenohumeral joint relies on tendons, ligaments, muscles and bony structures to provide stability. Shoulder stability is achieved by dynamically balancing the forces acting at the shoulder at any given time, including muscle contractile forces, fascial tension and external forces.
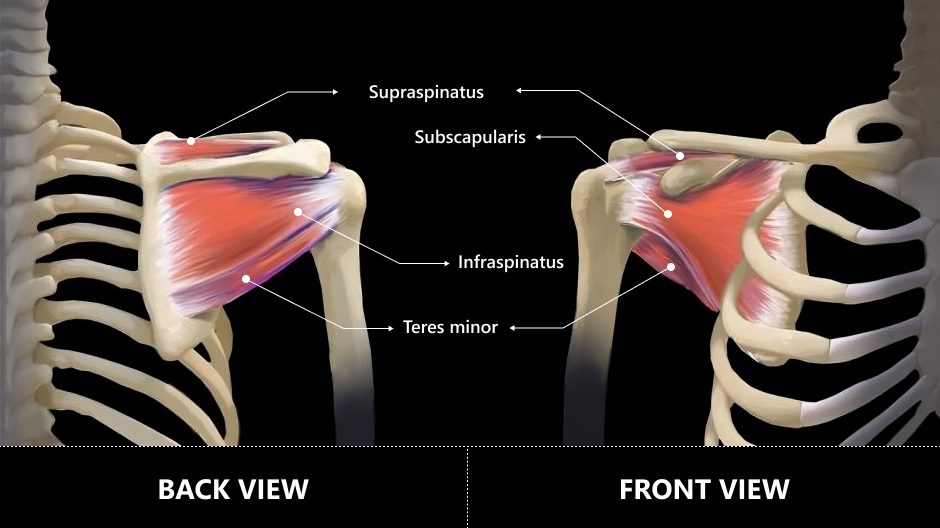
Muscles of the rotator cuff are:
The rotator cuff plays a key role in stabilizing the glenohumeral joint by compressing the head of the humerus (the ball) against the glenoid cavity (the socket). The tendons form a musculotendinous cuff around the front, back and top of the joint to keep the humerus from sliding out of place, allowing for full range of motion while at the same time providing stability.
The rotator cuff muscles also contribute to joint mobility by assisting in shoulder abduction, and medial and lateral rotation. The rotator cuff works in concert with a kinetic chain of 18 muscles that create a functional unit in the shoulder girdle complex. It works in conjunction with the deltoid muscle to balance the forces surrounding the glenohumeral joint
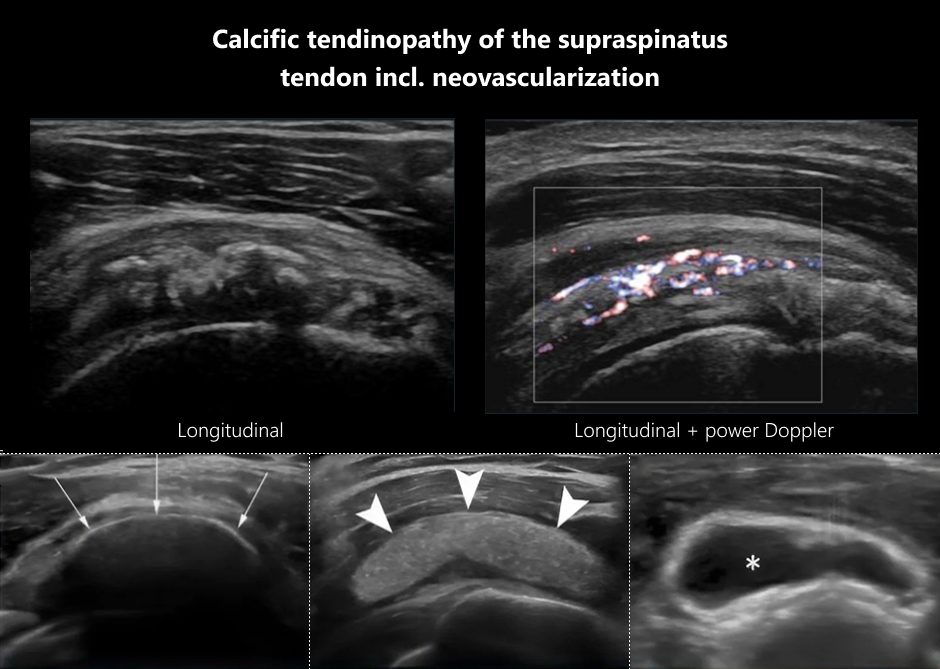
Shoulder calcific tendinopathy is a painful condition caused by calcium deposits in the rotator cuff tendons. Symptoms include persistent shoulder pain and stiffness with reduced joint range of motion. The specific factors that trigger calcific tendinopathy are as yet unknown, although researchers speculate that biological and genetic factors, along with lifestyle behaviors, likely play a role.
In about 80% of cases, the supraspinatus tendon is the site of calcification, followed by the infraspinatus at15 %, and the subscapularis at 5 %. About 70% of calcific tendinopathy patients are female, leading some researchers to suspect a hormonal influence. According to one study, patients with type 2 diabetes have a 27% increased risk of developing shoulder calcific tendinopathy within eight years after being diagnosed with diabetes.
Tendon calcification takes place in three distinct stages:
For decades, magnetic resonance imaging (MRI) has been the gold standard for diagnostic imaging. However, in addition to its inconvenience and expense, MRI has multiple disadvantages compared to high resolution diagnostic ultrasonography.

With ultrasound we can:
Traditional treatment of calcific shoulder tendinopathy includes:
However, conventional treatment approaches typically fall short of resolving the condition, and surgery should only be considered as a last resort after alternative treatment approaches have been exhausted.
New innovative approaches show greater promise for eliminating tendon calcification and restoring pain-free shoulder function, such as:

Ultrasound guidance of ESWT and needling procedures ensures that the therapies precisely impact the targeted tissues. Without ultrasound, such therapies can be inaccurate and less effective.
In addition, rehabilitation measures should address scapular dyskinesis, where the scapula’s position and range of motion is altered. Dyskinesis can arise from issues involving the shoulder itself, the cervical spine, and factors related to suboptimal posture. Scapular dyskinesis can cause subacromial impingement that contributes to shoulder pain.
Your shoulder joints are designed to move freely through multiple planes of motion, without pain or restriction. Seeking early treatment at the first signs of shoulder tendinopathy can dramatically reduce your symptoms and shorten your recovery time.
At NYDNRehab, we use the highest-resolution diagnostic ultrasound to visualize your shoulder in motion, in real time. Diagnosis takes place on your very first visit, in the comfort of our clinic, so we can start the rehabilitation process right away.
Don’t let shoulder pain keep you from doing the things you love. Contact NYDNRehab today, and restore healthy shoulder function with holistic personalized calcific tendinopathy treatment that really works!
Goetti, Patrick, et al. “Shoulder biomechanics in normal and selected pathological conditions.” EFORT open reviews 5.8 (2020): 508-518.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7484714/
Kalaycı, Cem Burak, and Eşref Kızılkaya. “Calcific tendinitis: intramuscular and intraosseous migration.” Diagnostic and Interventional Radiology 25.6 (2019): 480.
Calcific tendinitis: intramuscular and intraosseous migration
Martino, Gianluigi, et al. “Shoulder calcific tendinopathy.” Musculoskeletal ultrasound in orthopedic and rheumatic disease in adults. Cham: Springer International Publishing, 2022. 129-136.
Shoulder calcific tendinopathy
Sansone, Valerio, et al. “Calcific tendinopathy of the shoulder: clinical perspectives into the mechanisms, pathogenesis, and treatment.” Orthopedic research and reviews (2018): 63-72.
https://www.dovepress.com/calcific-tendinopathy-of-the-shoulder-clinical-perspectives-into-the-m-peer-reviewed-fulltext-article-ORR
Su, Yu‐Chi, et al. “Increased risk of shoulder calcific tendinopathy in diabetes mellitus: a nationwide, population‐based, matched cohort study.” International Journal of Clinical Practice 75.10 (2021): e14549.
https://onlinelibrary.wiley.com/doi/abs/10.1111/ijcp.14549

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































