Hip osteoarthritis (OA) is a degenerative joint disease marked by progressive loss of cartilage – the protective tissue that prevents smooth bone-on-bone gliding during movement. Once thought to be a natural symptom of aging caused by joint wear and tear, we now know that hip OA is a pro-inflammatory condition linked to various lifestyle factors. In its later stages, the loss of lubricating synovial fluid contributes to further progression of hip OA and degeneration of the joint.
New integrative therapies and technologies are now available to help combat hip OA by regenerating eroded cartilage, reversing the degenerative process, and restoring lubrication of the synovial capsule. When coupled with lifestyle modifications, holistic hip OA therapy can eliminate hip pain and restore pain-free functional movement.
or
Clinical director & DC RMSK
Verified Expert Profiles
NYDNRehab clinical director Dr. Lev Kalika has revolutionized hip osteoarthritis treatment using an integrative approach that combines high resolution musculoskeletal ultrasonography, cutting-edge therapeutic techniques and advanced technologies.
Dr. Kalika teams up with an orthobiologic injection specialist to provide ultrasound guidance for injection therapies and regenerative procedures, performed strategically at just the right time to promote tissue healing.
Dr. Kalika leverages multiple cutting edge therapies to treat hip OA, including:
When combined with personalized physical therapy and supported by research-grade technology, we are able to strengthen and stabilize patients’ hips, enabling them to tolerate load without pain while promoting the regeneration of protective cartilage.
Listen to Dr. Kalika’s podcast interview with AOR.US to learn more about his approach to hip osteoarthritis treatment: https://aor.us/podcasts/episode-75-bone-up-on-oa/.
At NYDNRehab, we treat hip OA with the most advanced, evidence-based approaches for hip cartilage regeneration. With over two decades of experience treating different types of arthritic and bone conditions, our multifaceted approach ensures that patients receive the most effective treatments currently available for hip OA therapy.
Hip OA therapy at NYDNRehab encompasses a holistic multimodal approach based on the most current scientific evidence. Our integrative approach goes beyond pain management to actually regenerating new cartilage to restore hip function.

Platelet-rich plasma (PRP) injections using the highest concentration of bioactive platelets, extracted from a sample of the patient's own blood. When the optimal dose of PRP is injected into the joint capsule, angiogenesis – the formation of new blood vessels – is promoted, fostering the growth of new cartilage.

Prolotherapy, a regenerative injection therapy that encourages the growth of new ligament and tendon fibers, resulting in tightened ligaments, enhanced joint alignment, improved stability and reduced muscle inhibition.

Extracorporeal shockwave therapy (ESWT), a non-invasive treatment approach that uses sound waves to stimulate biochemical activity in affected tissues.

Neuromodulation, a technique that uses electrical pulses to reduce pain by calming hyperactive nerves while stimulating supporting muscle action.

Stecco fascial manipulation to restore the elastic and slippery properties of fascia tissue. Healthy fascia provides elastic tension that supports the hip while enabling nerves and blood vessels to glide freely among other structures.

Fascial plane hydrodissection, to free up nerves entrapped by fascial densifications and adhesions.

Specialized physical therapy for hip OA to strengthen and balance the musculature of the hip and the entire lower kinetic chain.

To help clinicians diagnose and manage hip osteoarthritis, Professor Dietrich Tonnis and his colleagues developed a quantitative system of measurement for assessing hip dysplasia.
The Tonnis approach classifies osteoarthritic hips into the following categories:
Hip replacement surgery becomes an option when bones begin to touch and rub against each other. However, it is recommended that patients pursue and exhaust conservative interventions before opting for hip replacement.
Most people take everyday mobility for granted until an injury occurs or pain sets in. Sometimes pain and reduced mobility seem to arise out of nowhere, with no apparent cause or specific onset. Regardless of whether your pain is caused by trauma or by something less obvious, tensegrity plays a key role.
Tensegrity refers to tensile integrity – a state where a system of individual components is held together under continuous elastic tension. In the human body, tensegrity is created by the myofascial system, the network of muscles and fascia that work together to produce, control, and guide forces, and to hold the body’s various organs and structures in place during movement.
Tensegrity can be disrupted when myofascial tissues are injured or damaged in some way. When that happens, nerves and blood vessels can become entrapped, preventing them from gliding among other structures and producing pain. At the same time, the elastic tension that governs joint alignment and controls movement becomes compromised, creating motor deficits that undermine mobility and stability.
Factors that disrupt myofascial tensegrity include:
Many doctors do not understand the crucial role of the myofascial system in preventing pain syndromes, movement disorders, and disease. In fact, most medical doctors have no idea how to correct myofascial dysfunction or even recognize it as a factor. They simply treat pain symptoms with medications and eventually recommend surgery.
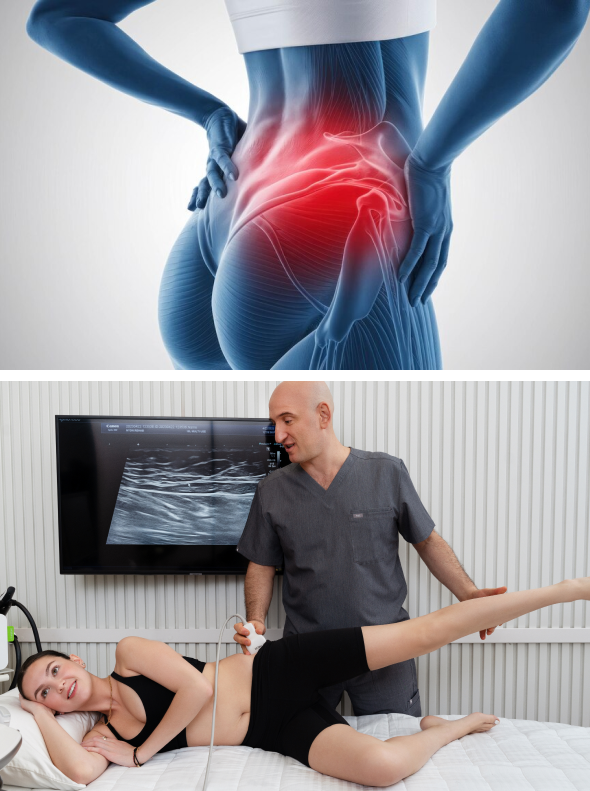
At NYDNRehab, we understand that the body’s systems work together as an integrated whole, and that treating pain is not enough to eliminate its source. We use dynamic high-resolution ultrasound to explore the myofascial system in real time. Ultrasound imaging lets us visualize muscles, fascia, nerves and other structures in motion, to identify places where tensegrity has been disrupted.
Once we identify the problem, we use the most advanced therapeutic approaches to restore myofascial integrity and promote tissue healing.
Click here to learn more about the causes of hip OA…
It has long been assumed that joint osteoarthritis is an inevitable consequence of aging. Yet multiple studies have proven that the true causes of joint degeneration in most people are sedentary lifestyles and obesity.
According to one recent study, the majority of hip OA hospitalizations can be prevented by attaining normal body weight and avoiding injury. Another peer-reviewed article debunks the notion of “wear and tear” as the underlying cause of joint OA.
Hip femoroacetabular impingement (FAI) and hip labrum tears are linked to the progression of hip osteoarthritis. FAI is a condition where extra bone grows along one or both bones that form the hip joint, giving them an irregular shape. A labrum tear can be painful and cause a sensation of the hip locking up, inhibiting range of motion. Surgical interventions for hip FAI and labral tears does not prevent patients from developing hip osteoarthritis.
Hip osteoarthritis is strongly associated with chronic systemic inflammation, prompting doctors to treat the condition with anti-inflammatory drugs, steroid injections, and viscosupplementation to replenish synovial hyaluronic acid and reduce friction. However, any evidence supporting those approaches is losing traction as new research exposes their limitations and adverse side effects.
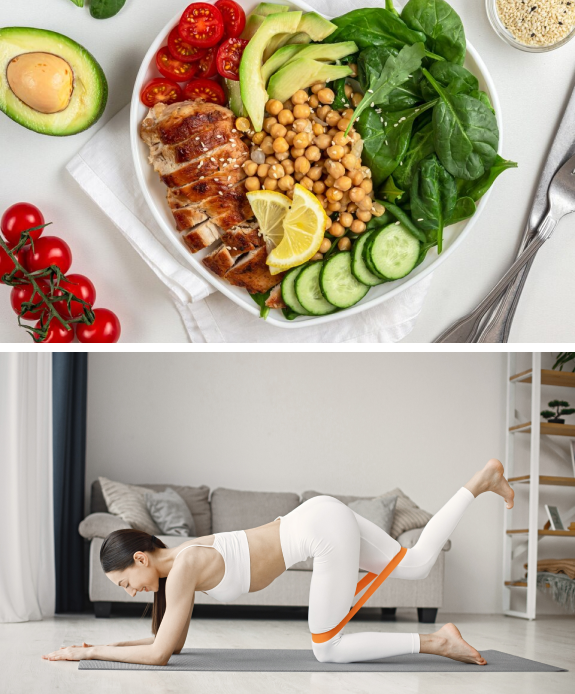
Recent research links the gut microbiome and its role in systemic inflammation to joint destruction and osteoarthritis, directly via intestinal dysbiosis, and indirectly via the promotion of metabolic syndrome and obesity. The gut microbiome can become disbiotic through poor diet, chronic dehydration, lack of exercise, and various antibiotics and medications. A diet high in fresh produce and fermented foods, and low in sugar and ultra-processed foods, can help restore a healthy gut ecosystem.
A 2021 review of scientific literature found that corticosteroid injections, while moderately effective for short-term pain relief, have multiple adverse side effects ranging from mild to severe.
Steroid negative side effects include:
In effect, any short-term benefits of steroid injections and viscosupplementation for hip OA are offset by potential long-term adverse effects that worsen the patient’s condition.
Identifying and treating underlying issues prior to beginning physical therapy is key to getting fast and effective results. Failure to pre-treat your condition can completely undermine your treatment protocol, and in some cases, your condition may even worsen.
Pretreatment, aka prehab, is also recommended prior to hip replacement surgery. Patients who undergo prehab typically have a shorter recovery time, and are more likely to regain full hip function.
Obstacles to physical therapy success include:
At NYDNRehab, we use a broad range of regenerative technologies and integrative therapeutic approaches to resolve issues that can stand in the way of successful physical therapy. Our staff is certified in a diverse array of holistic treatment methodologies, and our one-on-one treatment sessions are personalized, based on your unique diagnostic profile.
Once we pre-treat your damaged tissues and eliminate compensation patterns, your body will be ready to begin physical therapy.
The human body has its own innate healing mechanisms, but tissues sometimes need a nudge to accelerate the healing process. Regenerative technologies help to jump-start healing by stimulating tissue repair at the cellular level. Our outpatient regenerative therapies expedite recovery with minimal discomfort for the patient.

SoftWave is a groundbreaking regenerative mechanotransduction technology that accelerates tissue healing. Its patented electro-hydraulic applicator delivers high-speed soundwaves that can penetrate up to six inches in depth. SoftWave’s defocused and linear focused shockwaves recruit maximum stem cells to the treatment site to promote healing. SoftWave’s wider and deeper penetration using defocused energy is a preferred treatment option for a broad spectrum of conditions, ranging from orthopedic injuries to pelvic health. SoftWave is the only unfocused shockwave technology currently available. According to recent research, SoftWave defocused waves combined with focused and radial shockwaves have maximum regenerative potential.
MyACT is a new type of focused shockwave technology that allows for deeper compression of the focused waves. Its higher frequency allows for precise neuro modulation under ultrasound guidance, with a special linear head for treating myofascial pain. MyACT transforms the mechanical energy of shockwaves into biochemical signals that precisely target damaged tissues. Most injuries involve more than one tissue type. When used together, our advanced shockwave technologies enable us to specifically target multiple tissue types with the most effective shockwave treatment.


Focused ESWT is used as a regenerative treatment for damaged tendon, muscle and bone tissue. This technology produces high frequency sound waves to stimulate the body’s own reparative mechanisms. It is especially effective for chronic degenerative tendon disorders and myofascial pain syndrome.
EMTT transmits high energy magnetic pulses to targeted tissues that synchronize with the body’s own magnetic fields, triggering a regenerative response. EMTT waves can penetrate deep tissues to target difficult-to-reach tendons, muscles, bones and nerves.


EPAT, sometimes called defocused shock wave therapy, is not a true shockwave. It uses mechanical pressure waves to enhance blood circulation, improving oxygen and nutrient delivery to muscle and fascia tissues, but has minimal regenerative properties.The mechanical properties of EPAT make it especially effective for fascial manipulation in combination with focused shockwaves. We combine EPAT with different types of shockwaves for holistic treatment, without additional cost to the patient.
HEIT delivers high-intensity magnetic pulses to peripheral nerve tissues, to stimulate neuroplasticity. We leverage this FDA-approved methodology to treat pain and regenerate nerve fibers, for enhanced motor control.


INDIBA is a form of TECAR therapy that helps to restore the ionic charge of damaged cells, for faster injury healing and rehabilitation.
NESA generates a low-frequency electrical current of intermittent and cyclical stimuli that soothes hypersensitized nerves and restores optimal signaling between the autonomic nervous system and the brain. We leverage this FDA-approved methodology to treat pain and regenerate nerve fibers, to enhance motor control.

Injection therapies use orthobiologic solutions that stimulate cellular repair by either nourishing or irritating the targeted cells. Dr. Kalika teams up with an orthobiologic injection specialist, providing guidance by ultrasound to ensure that the injected substances hit their mark, for maximum effectiveness.

PRP therapy uses a sample of the patient’s own whole blood, which is spun in a centrifuge to extract a high concentration of platelets. When injected into damaged tissues, PRP initiates tissue repair by releasing biologically active factors such as growth factors, cytokines, lysosomes and adhesion proteins. The injected solution stimulates the synthesis of new connective tissues and blood vessels. PRP can help to jump-start healing in chronic injuries and accelerate repair in acute injuries.
Alpha 2 macroglobulin (A2M) is a naturally occurring blood plasma protein that acts as a carrier for numerous proteins and growth factors. As a protease inhibitor, A2M reduces inflammation in arthritic joints and helps to deactivate a variety of proteinases that typically degrade joint cartilage.
Prolotherapy uses a biologically neutral solution to irritate stubborn tissues, triggering the body’s innate healing mechanisms to grow new normal tendon, ligament and muscle fibers.
Hamstring injuries often involve fascial tissue that has become densified and/or formed adhesions, entrapping nerves and blood vessels, causing pain and restricting movement. Hydrodissection is a procedure where a saline solution is injected into densified fascia under ultrasound guidance. The solution works by separating fascial layers and freeing up entrapped nerves and blood vessels. We often use hydrodissection in conjunction with manual fascial manipulation.

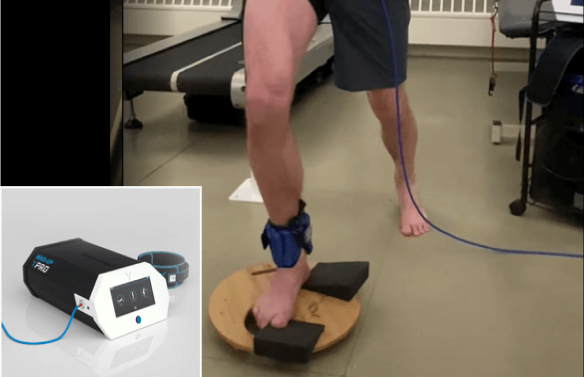
SM neuromuscular electrical stimulation (NMES) dynamically interacts with the patient during therapeutic exercises, providing real-time sensory, auditory and visual biofeedback to the patient. This breakthrough technology helps patients to recalibrate muscle actions, to optimize joint function. SMNMES has helped numerous patients to avoid unnecessary shoulder, knee and ankle surgeries, even in complex scenarios.
During PENS treatment, filament-thin needles are inserted through the skin into muscle tissue adjacent to the targeted nerve. A low frequency electrical current is then delivered via the inserted needles to stimulate the dysfunctional nerve. PENS normalizes nerve activity, improves brain plasticity and optimizes muscle recruitment patterns. This therapy is so effective that patients typically need only 4-6 treatment sessions.
Hip OA not only involves the degeneration of cartilage, but it is a chronic disease of the entire joint, affecting the cartilage, labrum, ligaments, fascia and muscles surrounding the hip. Its debilitating effects are strongly associated with metabolic disease and premature death.


Therapeutic exercises work to strengthen and rebalance the muscles that support the hip joint, taking pressure off of nerves and connective tissues, and realigning the joint for optimal function. Such exercises play a key role in restoring hip stability and eliminating factors that affect hip alignment. At NYDNRehab, we personalize your treatment plan based on your unique patient profile.
Once we have successfully pre-treated damaged tissues, we can begin one-on-one physical therapy to restore strength and stability, optimize mobility, and re-establish optimal neuromuscular pathways and muscle coordination patterns.

Your back-to-sports physical therapy protocol may include sport-specific training to optimize motor skills and restore peak athletic performance. We carefully monitor patient progress with ultrasound imaging to confirm complete recovery.
Advancements in technology are changing the game in rehabilitative medicine, enabling us to accelerate healing and restore performance at an unprecedented pace. The clinic at NYDNRehab features some of the most advanced therapeutic equipment currently available, and rarely found in private clinics.
Your knee OA therapy may include the use of high-tech equipment:



There are a number of things you can proactively do to prevent the onset of hip OA and halt its progression:
Request a gait analysis and gait retraining, to correct faulty gait mechanics that contribute to hip OA.
Medical doctors often attempt to manage your hip OA symptoms with drugs and surgery, without trying to heal and reverse the condition. The hip pain specialists at NYDNRehab are dedicated to resolving your hip OA by regenerating cartilage, promoting stability and restoring functional pain-free joint movement.
Our personalized one-on-one approach makes NYDNRehab the clinic of choice for hip OA in NYC. Contact us today, and get rid of debilitating hip pain so you can get back to doing the things you love.






























Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination



















