June 10, 2024

The human knee is a complex hinge joint made up of multiple structures, designed to withstand force loads many times the mass of the individual. But the knee’s complexity brings with it the potential for complicated injuries that are challenging to rehabilitate.
One of the most common knee injuries is a meniscus tear — a lesion or rupture of the rubbery discs that work as shock absorbers for your knee joint.
Learn about meniscus tears, and new technologies that deliver superior results over meniscus knee surgery.
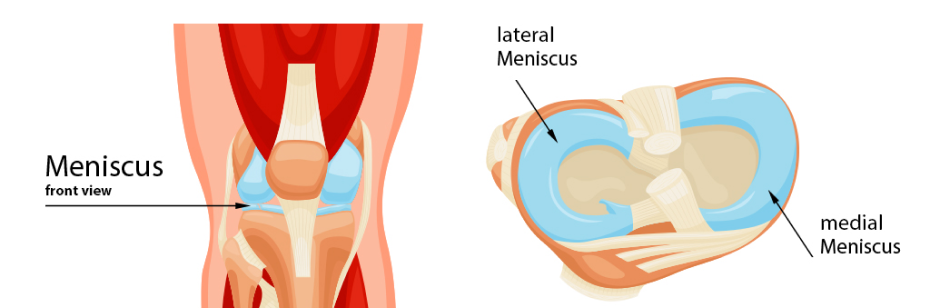
Each of your knees has two menisci — horseshoe-shaped structures of tough fibrocartilage that absorb shock and facilitate smooth gliding of your knee during physical activity. The medial meniscus is located on the inner side of the knee, and the lateral meniscus is on the outer side. The menisci attach to the tibia (shin bone) and provide stability for the knee during load transfer.
Biomechanical functions of the menisci include:
Menisci are made up of around 70 percent water, with cross-linked collagen fibers making up about 90 percent of their dry weight. Noncollagenous matrix proteins, such as fibronectin and elastin, make up the remaining 10 percent. Adequate hydration and nutritional support from foods that promote collagen synthesis can help to maintain the health and integrity of the menisci.
Like tendons and ligaments, the menisci are relatively avascular structures, with only a limited peripheral blood supply. When subjected to large force loads, lesions may arise that are slow to heal. Repetitive overload coupled with inadequate recovery time can increase the severity of lesions, resulting in major tears that cause pain and reduce performance. If left untreated, a torn meniscus can set you up for more serious injuries, like an ACL rupture.
Meniscus tears can be detected and confirmed with ultrasound or MRI. It is important to note that meniscus tears often occur in conjunction with other types of knee injuries, such as ACL ruptures and tibial plate fractures, or knee pathologies such as synovial inflammation, cartilage tears, and osteoarthritis. In such cases, meniscus surgery may have little effect on alleviating symptoms.
Symptoms of a meniscus tear include:
Risk factors for meniscus tears include:
Risk factors for meniscus tears include:

The location or a meniscus tear can be a key factor when prescribing treatment for a torn meniscus:
When a meniscus tear appears on MRI, many doctors are quick to recommend surgery. But in the majority of cases, unless the tear interferes with the mechanical function of the knee — e.g. flap tears — evidence indicates that meniscus surgery is rarely necessary, and that a torn meniscus can be effectively rehabilitated with physical therapy and alternative regenerative treatment.
Types of meniscus tears that may require surgery are:
Arthroscopic meniscus surgery is a fairly common procedure that removes or repairs damaged meniscus tissue. In cases of unstable tears that produce knee locking or catching, surgery may be necessary. However, the vast majority of meniscus tears do not require surgical intervention. In fact, it is recommended that 98% of meniscus tears be treated conservatively.
Meniscus tears do not always cause mechanical symptoms, and a partial meniscectomy where tissue is removed can actually worsen knee mechanics by reducing the ability of the meniscus to mediate weight-bearing stress. This can alter knee biomechanics and cause unfavorable compensation patterns that affect gait and undermine performance. Removal of meniscus tissue can also cause early-onset knee osteoarthritis.
For athletes, lateral meniscectomies significantly reduce return-to-play rates, and lateral meniscus tears can be more career-threatening than ACL injuries.
A recent study (6) looked at 102 middle-aged patients, 5 years post meniscus treatment. The patients had been randomly assigned to one of two treatment groups: meniscus surgery plus exercise therapy, or exercise therapy alone. The researchers found that surgery provided no additional long-term benefit after 5 years compared with exercise alone, and that radiographic images did not differ between the two groups.
Another cross-sectional study (5) of 566 middle-aged patients who had meniscus surgery challenges the appropriateness of arthroscopic surgery based on patient-reported mechanical symptoms of knee locking, catching, or limited range of motion. The researchers found that for large numbers of patients, meniscus surgery did nothing to relieve mechanical symptoms. One study found that patients undergoing meniscus surgery fared no better than cohorts who underwent a sham surgery. The researchers noted that meniscus tears often coincide with other knee pathologies such as synovial inflammation, cartilage lesions and osteoarthritis, which may be the cause of mechanical symptoms.
A third study (2) looked at 121 younger patients (aged 18-40) to compare the outcomes of meniscus surgery vs 12 weeks of exercise therapy plus education. The researchers concluded that early surgery appeared to be more effective in relieving self-reported mechanical knee symptoms, but that surgery did not improve patients’ pain, function or quality of life.
A fourth study (3) looked at data from 565 patients diagnosed with meniscus tears and concomitant knee cartilage damage. The researchers found that cartilage damage was strongly associated with significantly worse patient-reported knee symptoms. They found no such association between patient-reported symptoms and meniscus damage. They concluded that mechanical symptoms were most likely caused by cartilage damage, and not by meniscus tears.
In addition to exercises aimed at strengthening the knee’s supporting structures, there are a number of alternative regenerative treatment and injection therapies that can stimulate and accelerate the healing of meniscus tears. Regenerative approaches tap into the body’s own innate healing mechanisms, to jump-start and speed up the healing process.
ESWT is proven to be an effective regenerative treatment for damaged meniscus tissue. This technology produces high frequency sound waves to stimulate the body’s own reparative mechanisms. One recent study (4) conducted on rats found that ESWT promoted meniscal tear healing in the avascular area by stimulating cell proliferation and sparking the upregulation of cartilage-repairing factors.
EMTT is used to transmit high energy magnetic pulses to damaged meniscus tissues. The magnetic waves synchronize with the body’s own magnetic fields, causing a disturbance that triggers a regenerative response.
When used together, ESWT and EMTT form a dynamic duo that accelerate the repair and healing of meniscus tears.

Ultrasound guided injection therapies also trigger a regenerative response in torn meniscus tissue.
injects a biologically neutral solution to irritate the meniscus tissue, triggering the body’s natural healing mechanisms.
injects platelets extracted from the patient’s own blood into the meniscus, releasing biologically active factors that promote tissue repair.
is an advanced treatment for more complex and traumatic meniscus tears. Stem cell therapy recruits growth factors in the injured area and enhances stem cell activity for meniscus cell regeneration.
Meniscus tears can be career-ending for athletes and can dramatically impact the quality of life of older adults. Surgery of any type has inherent risks. Patients should carefully weigh the side effects of drugs and anesthesia, risk of infection, high costs, disappointing outcomes and long-term complications of surgery vs low-risk alternatives. If you do opt for surgery, you will still need physical therapy to rehabilitate your knee and restore functional movement.
At NYDNRehab, we use high-resolution diagnostic ultrasound to get a clear picture of the location, type and extent of injury to your meniscus. Our treatment toolbox features the most advanced meniscus tear therapies available, to repair and rehabilitate your meniscus injury so you can return to physical activity and daily life with confidence.
Resources
1. Adams, Bryan G., Megan N. Houston, and Kenneth L. Cameron. “The epidemiology of meniscus injury.” Sports medicine and arthroscopy review 29.3 (2021): e24-e33.
2. Damsted, Camma, et al. “Effect of exercise therapy versus surgery on mechanical symptoms in young patients with a meniscal tear: a secondary analysis of the DREAM trial.” British Journal of Sports Medicine 57.9 (2023): 521-527.
3. Farina, Evan M., et al. “Meniscal and mechanical symptoms are associated with cartilage damage, not meniscal pathology.” JBJS 103.5 (2021): 381-388.
4. Hashimoto, Shogo, et al. “Extracorporeal shockwave therapy accelerates the healing of a meniscal tear in the avascular region in a rat model.” The American Journal of Sports Medicine 47.12 (2019): 2937-2944.
5. Pihl, Kenneth, et al. “Association of specific meniscal pathologies and other structural pathologies with self-reported mechanical symptoms: A cross-sectional study of 566 patients undergoing meniscal surgery.” Journal of Science and Medicine in Sport 22.2 (2019): 151-157.
6. Sonesson, Sofi, et al. “Knee arthroscopic surgery in middle-aged patients with meniscal symptoms: a 5-year follow-up of a prospective, randomized study.” Orthopaedic journal of sports medicine 8.1 (2020): 2325967119893920.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































