
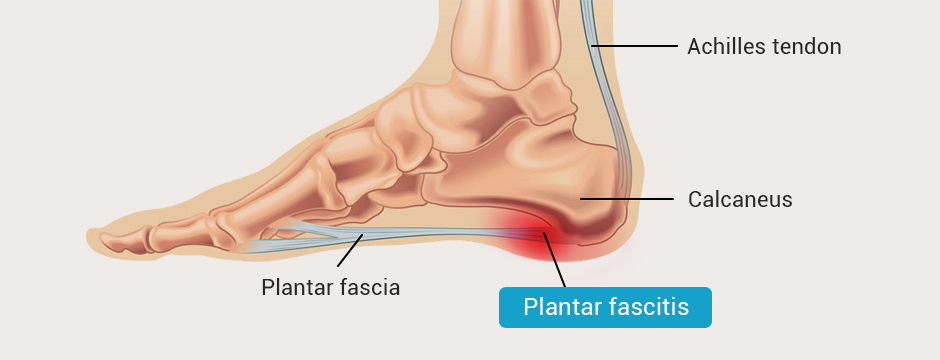
The plantar fascia is a tough band of connective tissue that connects your heel to your toes. During walking, running and jumping, the plantar fascia stores energy as it stretches, releasing it as it recoils to contribute to force production – an action known as the windlass mechanism.
Plantar fasciitis is a common overuse injury that is first felt as heel pain. As the condition worsens, pain may radiate from the heel along the entire foot arch, where the plantar fascia spans from heel to toe.
Plantar fasciitis symptoms include:
Sharp pain on the bottom of the heel
Pain that worsens after, but not during, exercise
Pain along the foot arch
Pain that worsens after sleeping or sitting for long periods
Swelling in the heel
Tightness in the Achilles tendon
Ongoing heel pain that lasts for weeks or months.
Runners, athletes and fitness enthusiasts are all vulnerable to plantar fasciitis. The condition is also common among people who walk or stand for long hours, especially on concrete. Certain types of footwear, like flip-flops and high heels, may also contribute to plantar fasciitis.
Your body is designed to heal itself, but the healing process takes time, and without professional intervention, damaged tissues may not heal in ways that restore optimal function. To get fast and enduring results that restore pain-free functional movement, you need the help of skilled and experienced specialists, trained and certified in cutting-edge therapies.
Whether you are an athlete suffering an injury, a patient recovering from surgery, or you are experiencing pain and impaired movement, you deserve the best treatment available.
Conventional treatments for plantar fasciitis include:
Ice and NSAIDS to reduce pain and inflammation
Orthotics designed to reduce stress on the plantar fascia
Discontinuation or reduction of activity
Therapeutic massage and athletic taping
Corticosteroid injections
Foam rolling
Stretching
Surgery (as a last resort)
The plantar fascia (PF) is only one of many structures that make up the foot and ankle complex, none of which functions independently of the others. Treating the locus of pain without addressing the mechanical and structural components of the entire lower kinetic chain can prolong plantar fasciitis, wasting the patient’s time and money without fully resolving their condition.
Factors that contribute to plantar fasciitis include:
Compensation for former or current injuries that overloads the plantar fascia on one side of the body
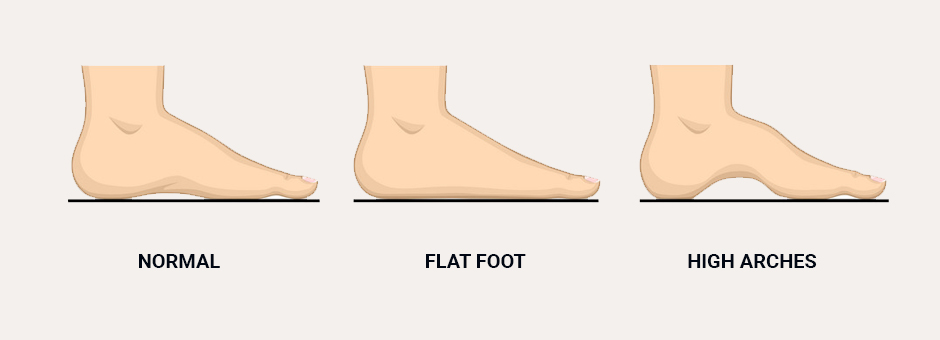
Unusually high arches or flat feet
Tight hamstring muscles that force the PF to work harder
Tight Achilles tendon that forces the PF to over-stretch
A rigid big toe that causes the plantar fascia to overstretch during the push-off phase of the gait cycle, inhibiting the windlass mechanism
While plantar fasciitis treatment should address pain, therapy should not stop there. Gait should be analyzed to assess for motor deficiencies. Range of motion of the leg joints and muscles should also be assessed, and flexibility training should be prescribed to address tightness in the hamstrings and Achilles tendon.
Stretching is often prescribed as first-line treatment for plantar fasciitis. But considering that overstretching of the plantar fascia is a key contributing factor to plantar fasciitis, additional stretching as a treatment approach can actually worsen the condition. An overstretched PF can inhibit the foot from supinating, causing stress where the plantar fascia inserts at the heel.
Any decision to stretch the plantar fascia should be based on high-resolution diagnostic ultrasound imaging, which is superior to MRI in that it allows the clinician to visualize multiple structures that may contribute to PF pain.
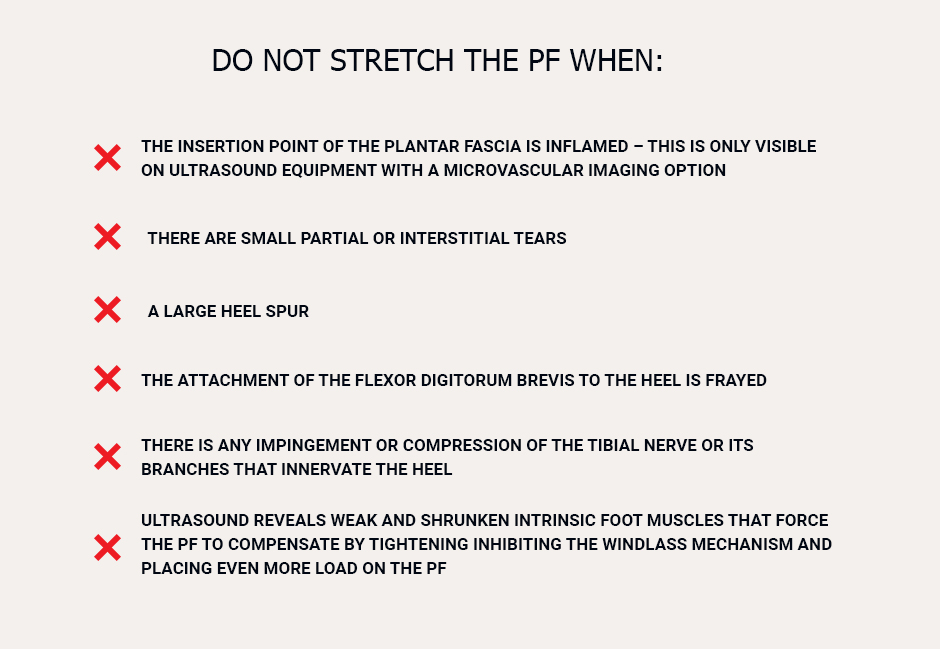
Do not stretch the PF when:
The insertion point of the plantar fascia is inflamed – this is only visible on ultrasound equipment with a microvascular imaging option
There are small partial or interstitial tears
There is a large heel spur
The attachment of the flexor digitorum brevis to the heel is frayed
There is any impingement or compression of the tibial nerve or its branches that innervate the heel
Ultrasound reveals weak and shrunken intrinsic foot muscles that force the PF to compensate by tightening, inhibiting the windlass mechanism and placing even more load on the PF
Stretching may be effective if:
Ultrasound reveals hypertrophied (enlarged) plantar intrinsic muscles
The PF is uniformly thickened, with no tears or inflammation
Recent research by Rathleff et al. (2015) suggests that high load strength training may speed up recovery from plantar fasciitis more quickly than stretching alone.
In medicine, the suffix “itis” refers to inflammation, and the term “fasciitis” can be a misnomer. When it comes to connective tissues like fascia, tendons and ligaments, inflammation is uncommon due to the limited vascularity of connective tissues.
In the case of plantar fasciitis, pain is often attributed to micro tears along the PF caused by overstretching. Limited vascularity causes healing to progress slowly due to poor delivery of nutrients and oxygen to the damaged tissues. In addition, trigger points – tiny knots of tightly contracted muscle fibers – can intensify plantar fasciitis pain.
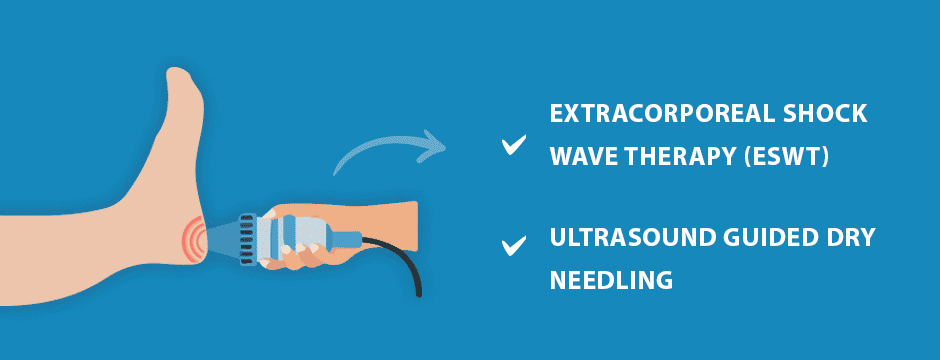
At NYDNRehab, we leverage new technologies to speed healing of the PF:
Extracorporeal shock wave therapy (ESWT) applies high frequency sound waves to the damaged PF, to stimulate the body’s own reparative mechanisms. ESWT is especially effective for jump-starting the healing process in slow-to-heal connective tissues. Patients often report pain relief after a single session, and total recovery after several sessions.
Ultrasound guided dry needling uses thin non-medicated needles to penetrate myofascial trigger points that often contribute to PF pain. The needles evoke a twitch response in the muscle fibers that causes them to relax, providing immediate pain relief.
Additional treatment modalities may include:
Gait analysis and retraining
Rehabilitation of old and/or new injuries
Manual therapy
Other regenerative therapies
Strength training of the intrinsic foot muscles
Stretching of the hamstrings and Achilles tendon
Accurate diagnosis of plantar fasciitis is fundamental to successful treatment. Patients are frequently misdiagnosed and treated for plantar fasciitis, when heel pain is often caused by other conditions that share similar symptoms.
At NYDNRehab, we use the highest resolution diagnostic ultrasound equipment to visualize the structures of the foot, ankle and lower extremity in real time. Our equipment also gives us the capability of microvascular imaging, to identify inflammation of the PF.
After a thorough assessment and diagnosis, we create a personalized one-on-one treatment plan, based on your unique profile. Our goal is to eliminate PF pain at its source, and as quickly as possible, so you can enjoy your life to its fullest.
Resource
Adams, Bryan G., Megan N. Houston, and Kenneth L. Cameron. “The epidemiology of meniscus injury.” Sports medicine and arthroscopy review 29.3 (2021): e24-e33.
Borque, Kyle A., et al. “Evidence-based rationale for treatment of meniscal lesions in athletes.” Knee Surgery, Sports Traumatology, Arthroscopy (2021): 1-9.
Giuffrida, A., et al. “Conservative vs. surgical approach for degenerative meniscal injuries: a systematic review of clinical evidence.” Eur Rev Med Pharmacol Sci 24.6 (2020): 2874-2885.
Reito, Aleksi, Ian A. Harris, and Teemu Karjalainen. “Arthroscopic partial meniscectomy: did it ever work? A narrative review from basic research to proposed disease framework and science of clinical practice.” Acta orthopaedica (2021): 1-10.

























Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















