
Most sports fans understand that an ACL rupture can be a death blow to any athlete, taking them out of the game for the season and possibly ending their career. For elite athletes, injuries are a high-stakes risk, with millions of dollars hanging in the balance. In the US, reconstructive surgery is almost a given when an athlete ruptures an ACL, despite mounting evidence that surgery is not always the best option.
In youth athletics, early ACL surgery can disrupt the growth plate, interfering with proper bone development. In many cases it is advised to avoid surgery until the bones stop growing. Young athletes who suffer ACL injuries are likely to experience knee osteoarthritis in their 20s and 30s, resulting in chronic pain and reduced knee function.
To date there is no research that demonstrate that ACL reconstructive surgery lowers the risk of knee osteoarthritis, and one study found that patients who had ACL reconstruction experienced higher levels of knee osteoarthritis than those who had conservative care only.
Determining when an athlete needs surgery and when conservative care is a better option poses a difficult decision for coaches, athletes, parents and medical personnel.
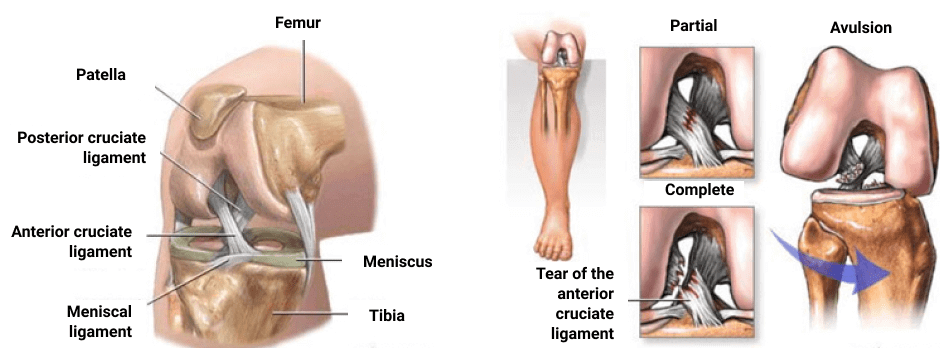
The anterior cruciate ligament, or ACL, plays an important role in knee stability, especially in high-intensity sports that involve jumping, landing, pivoting, cutting and rapid directional changes. The ACL, along with other knee ligaments, helps prevent the knee from sliding, rotating or hyperextending during vigorous physical activity.
Symptoms of an ACL injury include:
ACL injuries are not common among the general population, but they are quite common among athletes of both genders, and female athletes are at a higher risk than males. Continuing to play sports with an untreated ACL injury can increase the severity of the injury, and increase the athlete’s risk of injury to knee cartilage and menisci.
There is much controversy surrounding the topic of surgical vs conservative treatment of ACL ruptures, and some research indicates that surgery is no more beneficial for certain patients than non-surgical care. At the end of the day, it is up to patients, coaches and medical professionals to determine what is best for the individual athlete.
One approach in decision making involves categorizing patients as either “copers” or “non-copers.”
ACL patients who fall under the “coper” category are able to function in certain activities despite their injuries. The knee in copers is fairly stable compared to non-copers, whose injured knee tends to repeatedly give way. Copers are considered to be good candidates for conservative care, without reconstructive surgery. Non-copers should undergo at least 3 months of prehab, prior to reconstructive surgery.
The challenge is to sort copers from non-copers, to determine the best treatment path for the individual athlete. For that purpose, certain tests can be conducted to assess knee stability in ACL injuries.
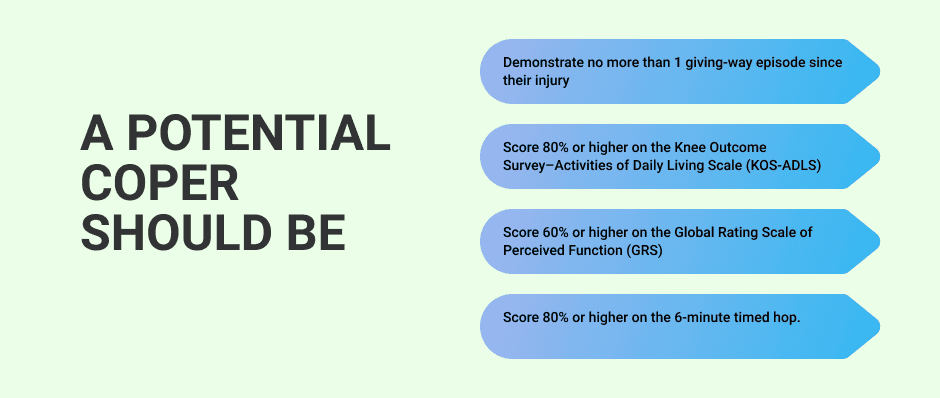
A potential coper should be able to:
Once a patient has been categorized as a coper or non-coper and has undergone the initial phase of rehabilitation, decision-making shared among all stakeholders, including the athlete, will determine whether to continue on a conservative treatment path, or whether surgical reconstruction offers the best outcome.
Professional athletes have the advantage of trainers and coaches dedicated to helping them excel at their sport. They spend long hours training to strengthen and stabilize the structures surrounding the knees, to improve performance and decrease injury risk.
According to the American Academy of Pediatrics, sport-specific training can reduce a young athlete’s risk of ACL injury by as much as 72%. However, youth athletic programs often lack the resources to provide the caliber of training necessary to prevent knee injuries. Young athletes who are serious about their sport would benefit from a sports physical therapy training program to optimize performance and minimize injury risk.
The sports medicine team at NYDNRehab treats every patient as a unique individual. We never take a one-size-fits-all approach to ACL treatment. With state-of-the art technologies and innovative treatment methods at our disposal, we collect quantitative data and apply it in our recovery protocols. Whether you need prehab, rehab or simply need to strengthen and stabilize your knees, NYDNRehab is the best sports medicine rehab clinic in NYC.
Resources
LaBella, Cynthia R., William Hennrikus, and Timothy E. Hewett. “Anterior cruciate ligament injuries: diagnosis, treatment, and prevention.” Pediatrics 133.5 (2014): e1437-e1450.
Thoma, Louise M., et al. “Coper classification early after anterior cruciate ligament rupture changes with progressive neuromuscular and strength training and is associated with 2-year success: the Delaware-Oslo ACL Cohort Study.” The American journal of sports medicine 47.4 (2019): 807-814.
Wellsandt, Elizabeth, et al. “Does anterior cruciate ligament reconstruction improve functional and radiographic outcomes over nonoperative management 5 Years after injury?.” The American journal of sports medicine 46.9 (2018): 2103-2112.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































