Nearly 30 years ago, Dr. Martha Murray’s life was changed; she met a man using crutches as a Stanford party, discussing his ACL tear. After informing Murray his surgery would involve drilling holes into the bones and grafting a tendon, she was taken aback and wondered why the two ligaments couldn’t just be sewn together and left to heal.
Since then, she’s been deeply involved in ACL tears, looking for new methods of treatment for an ACL tear and how to prevent ACL tears in the future. The result of her hard work? Ready for testing is a new sponge scaffold that can completely change how human knees heal.
If the human trials work out well, then the spongy alternative could provide a new option for athletes in need of less invasive surgery and shorter recovery times. This is especially true for the athletes Murray commonly sees at her office in the Division of Sports Medicine at the Boston Children’s Hospital.
Each year, nearly 400,000 people suffer an ACL injury, producing symptoms of pain and other similar symptoms of ACL tear, just in the United States. Woman are two to six times more likely to suffer such an injury compared to a male who plays the same sport. In other words, Murray’s work could help thousands. She took the time to explain how she went from faithful engineering student to a dedicated healer of ACL tear, meniscus tear and similar damages to the knee ligaments.
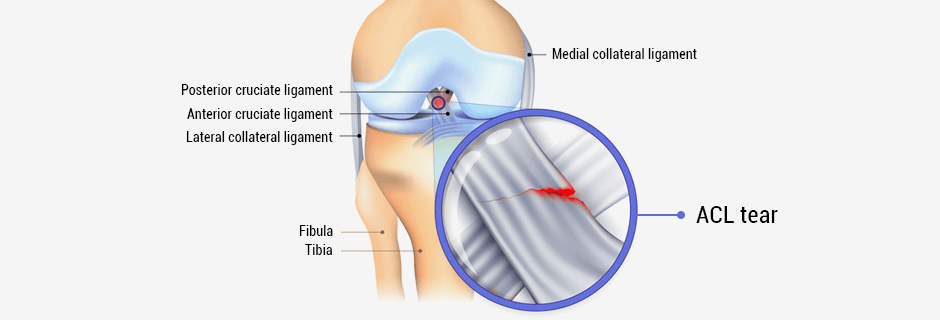
After the medial collateral ligament (MCL) tears, both ends bleed, causing a natural scaffold bridging the two together until it can properly heal itself. In an ACL tear, the torn ends will bleed but the blood can’t clot because of joint fluid. You end up with two bad ends that sit in this fluid instead of reconnecting with each other.
After that, a spongy scaffold was designed that can hold the blood between the two injured points. It can remain long enough so the cells grow in it, repairing itself enough to be removed after six to eight weeks once sufficient healing tissue has grown.
The FDA recently approved the scaffold for testing in 10 patients. It’s known as a safety study, which is phase zero if anything. This is where you make sure no major red flags come up that were absent from preliminary testing.
Patients between the ages of 18 and 35 years old whose injury was recent are needed, as in the last week or two. Unfortunately, after an ACL tear, the ligament starts to degrade, need new options. Patients with recent symptoms who may be interested qualify.
As it stands, ACL tear reconstruction is effective procedure. Most patients have no problem returning to sports. However, especially with teenagers, there is a good risk of tearing the graft that was used to repair it — about 20 percent. It is impossible to prevent arthritis in the joint as well after reconstruction. It’s important to stop this as many of patients are between 15 and 20 years old. If they develop the condition later, they’ll be in their 30s with a bad knee.
With the animal trials, the ones repaired didn’t seem to have arthritis in the same way that those with reconstructions or lack of treatment developed. As such, it’s optimal symptoms can be eliminated and an effective treatment with minimal recovery downtime and the ability to prevent arthritis can be provided. It is hoped this will be the better long-term option for those with a sprain, damaged anatomy, meniscus tear symptoms, knee pain or otherwise in need of ACL repair.
The goal is to stop the thought of replacing our damaged anatomy with metal, synthetics or anything else. We as a society need to instead take advantage of the benefits our own anatomy gives us, using our evolutionary biology to heal our own tissue. Whether it’s meniscus, a sprain, torn ligaments or an ACL tear, you should heal better.
In orthopedics, if you consider the meniscus, ligaments and cartilage — all tissues that do not heal — all of them live within joints. They all suffer from the issue not getting an initial scaffold. One must get rid of them or trim them since they don’t heal on their own. If that can be added to that scaffold with the right biological cues, the tissues can be saved.
Perhaps it is not yet the final solution. However, scientists believe in the cause, then they could develop an even more efficient one or add some better growth factor down the line.
Advice was sought from various physical therapists who have experience in ACL, sprain and meniscus rehabilitation treatment. They were informed of the project and worked to come up with a protocol not unlike what would occur following an ACL graft. The goal is to progress through and fine tune the protocol so it starts with easy activities and end with harder ones to minimize pain. Time will tell if this is successful — will it be too aggressive or perhaps not enough for the patient?

Three months into recovery, an MRI of the knee is taken and factor in any pain they are having. New techniques will let doctors see see how strong the repair is and whether or not it’s working early on. If they are not seeing success, they can have reconstruction.
NYDN Rehab clinic offers various most advanced treatment options for those suffering from ACL tears and similar injuries in Manhattan and the surrounding boroughs. From ACL pain and orthopedic issues to back, neck, wrist and elbow pain, you can find effective treatment through the NYDNRehab clinic.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































