
There is a lot going on in your pelvic region, and therefore a lot that can go wrong. In addition to housing and protecting your eliminatory and reproductive organs, your pelvic muscles play a critical role in gait, balance, and load transfer during sports and everyday movement.
Unstable pelvic motion in the frontal plane, where adduction and abduction take place, can undermine sports performance and reduce walking and running gait efficiency. If left untreated, frontal pelvic instability can lead to injuries with long-term repercussions. Many things can contribute to frontal plane instability, and accurate diagnosis is critical for effective treatment.
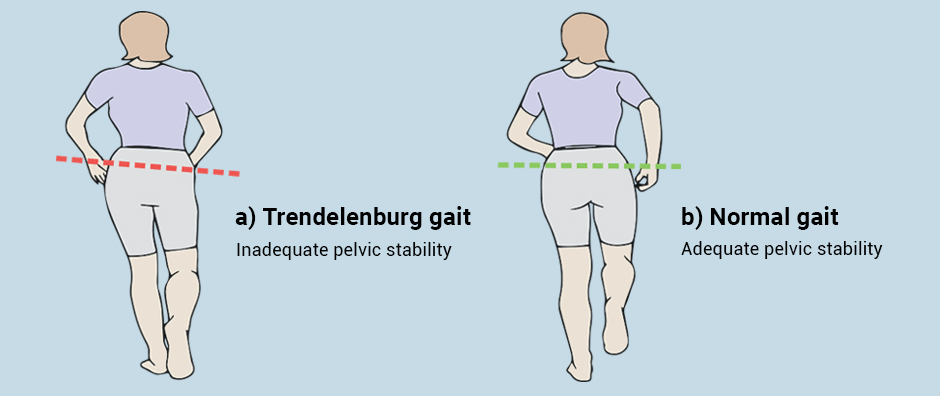
Your pelvic muscles play a key role in walking and running gait. Muscles in your pelvic region control balance, transfer force loads between your lower and upper body, and enhance energy efficiency during the gait cycle. During the gait cycle, your pelvis tilts downwards on the non-weight bearing side. Your body compensates by tilting the trunk laterally (to the side), away from the dropped hip, shifting your center of gravity to your weight-bearing limb and offsetting pelvic drop. When the pelvis is unstable, the mechanisms of load transfer are less efficient.
In both athletes and the general population, frontal plane pelvic femoral instability is an important common denominator in multiple low back, hip, knee, foot and ankle conditions. Until recently, frontal pelvic instability was thought to be caused by weakened posterior hip abductors and external rotators, especially the gluteus medius muscle, but recent research has identified other contributing factors.
In terms of rehabilitation, strengthening specific muscles in isolation is not likely to have a significant global impact on whole-body gait mechanics, and only a small impact on overall pelvic stability. Although the gluteus medius plays a primary role in lateral hip stability during gait, strengthening the gluteus medius alone has only a small effect on pelvic drop kinematics. During load transfer to your weight-bearing leg, you also engage your oblique abdominal muscles and the quadratus lumborum of your lower back. In addition, timing between the foot muscles that control subtalar deceleration in the frontal and transverse planes, and engagement of the hip and core muscles in the frontal plane appears to play a role.
Here are some recent findings on gait kinematics and pelvic instability:
If you are a walker or runner and suffer from low back, hip, knee or pelvic pain, you may have frontal plane pelvic femoral instability. In addition to a physical exam that evaluates your hip and pelvic alignment, there is a broad range of clinical tests and assessments for hip range of motion, balance and muscle strength.
One of the most effective ways to assess pelvic stability is 3D gait analysis, that lets us evaluate your hip and pelvic movement in all three planes of motion.
At NYDNRehab, our high-tech gait analysis lab features some of the most advanced technology for diagnosis and rehabilitation:
One of the greatest advantages of incorporating technology into diagnosis and rehab is its ability to provide quantitative data on movement kinematics. By quantifying your biomechanical parameters, we are able to precisely gauge your progress and make adjustments in your treatment plan accordingly. In addition, we use artificial intelligence (AI) technology to provide real-time feedback, to enhance and accelerate the rehab process.
Pelvic pain or pain in other areas of your body from running is not natural, and ignoring it will only lead to more pain and injury. Assessing your gait mechanics and giving them a tuneup can make a world of difference in how you walk and run. A 3D running gait analysis at NYDNRehab can reveal hidden causes of pain and discomfort, and can head off future injuries. Don’t give up running because of pain. Get to the source of pain and eliminate it with the sports medicine team at NYDNR.
Resources:
Cruz, Aline de Castro, et al. “Pelvic drop changes due to proximal muscle strengthening depend on foot-ankle varus alignment.” Applied bionics and biomechanics 2019 (2019)
Kararti, Caner, et al. “Are Biomechanical Features of the Foot and Ankle Related to Lumbopelvic Motor Control?.” Journal of the American Podiatric Medical Association (2019): 0000-0000.
Noehren, B., J. Scholz, and I. Davis. “The effect of real-time gait retraining on hip kinematics, pain and function in subjects with patellofemoral pain syndrome.” British journal of sports medicine 45.9 (2011): 691-696.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































