Our patient is a 56 year-old male jeweler who came to us with lateral elbow pain. The patient is a very athletic tennis player who works out at the gym on a regular basis. He stated that his pain initially started at the front of his elbow and eventually moved toward his lateral epicondyle, where he pointed out a tender spot.
The patient had seen an orthopedist who referred him for an MRI. After review of his MRI, he was told that his pain was muscular and surgery would not help. He was referred for physical therapy, with no results after four months of treatment.
We conducted a neurological exam to rule out cervical involvement. We identified restricted elbow range of motion during extension, pronation and supination. Palpation of the epitrochlear groove of the ulnar nerve revealed no tenderness of the supinator muscle, and we were able to rule out nerve compression at the arcade of Frohse.
There was tenderness at the insertion of the common extensor tendons and the lateral epicondyle. There was no pain with resisted wrist extension, but the soft tissues of his dorsal wrist felt thickened, especially around the carpal retinaculum. Upon closer examination of his wrist we discovered limited wrist extension, along with some hypermobility and pain in his first metacarpophalangeal joint.
We began our ultrasound exam by tracing the radial and posterior interosseous nerves, since their entrapment in the arcade of Frohse or in the radial tunnel can mimic lateral epicondylitis. These nerves are difficult to visualize with MRI, and their dynamic entrapment cannot be detected with MRI.
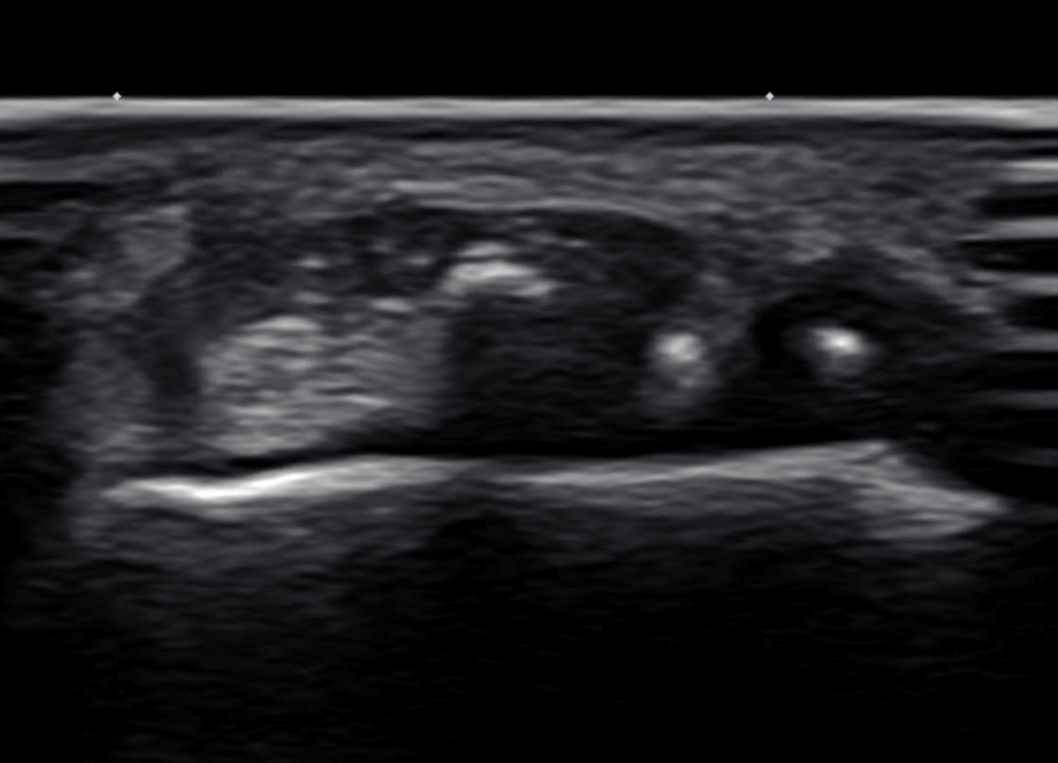
The nerves appeared normal in terms of their size and echogenicity along the entire length of the arm and forearm. There was no encroachment on the nerves during dynamic maneuvers. Despite a normal appearance of the distal biceps tendon on MRI, we found some changes in echogenicity of the distal short head of the biceps, with some enthesopathy that could explain his initial symptoms.
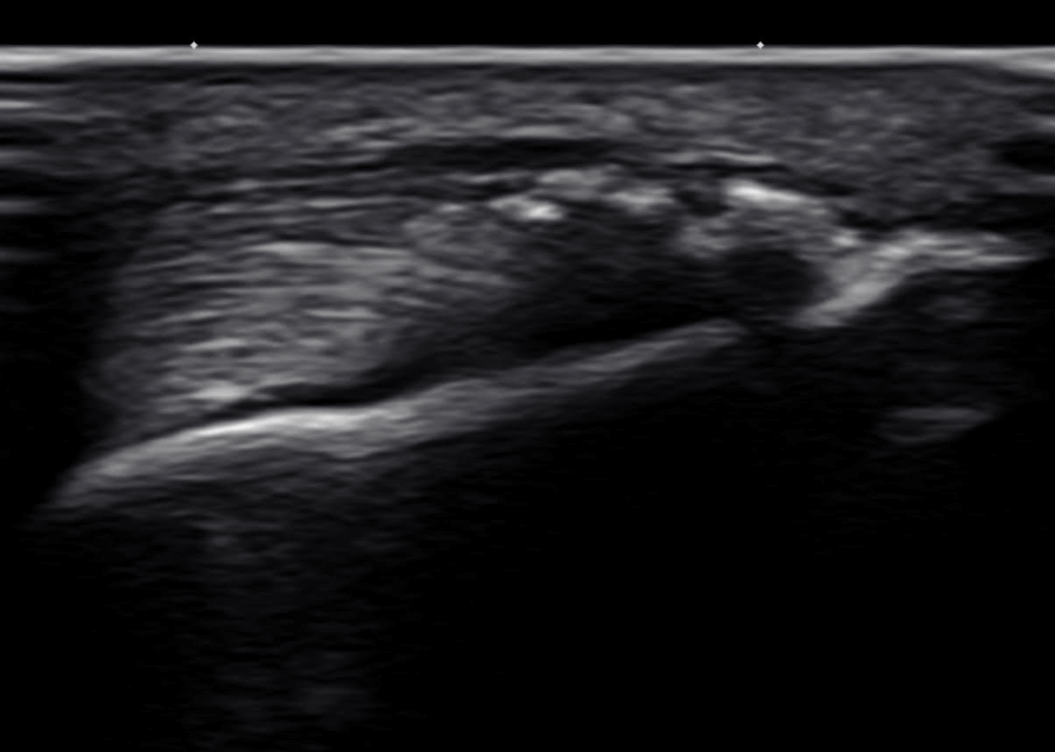
During dynamic examination of the ulnar nerve with elbow flexion, the patient complained of mild pain in his olecranon – the bony prominence of the elbow at the upper end of the ulna. When we visualized his distal tendon attachment, we found triceps tendinopathy.
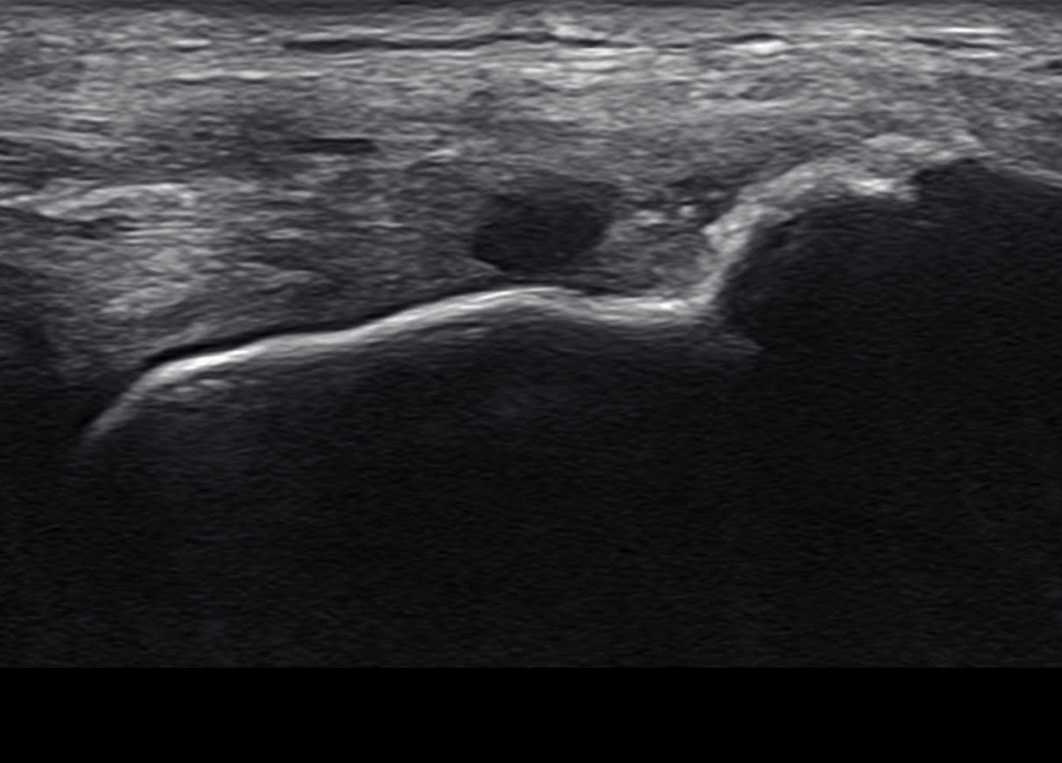
We then examined the common extensor tendon attachments to the lateral epicondyle and found a small partial thickness tear in the deep portion of the extensor carpi radialis brevis (ECRB), which was not visible on MRI.
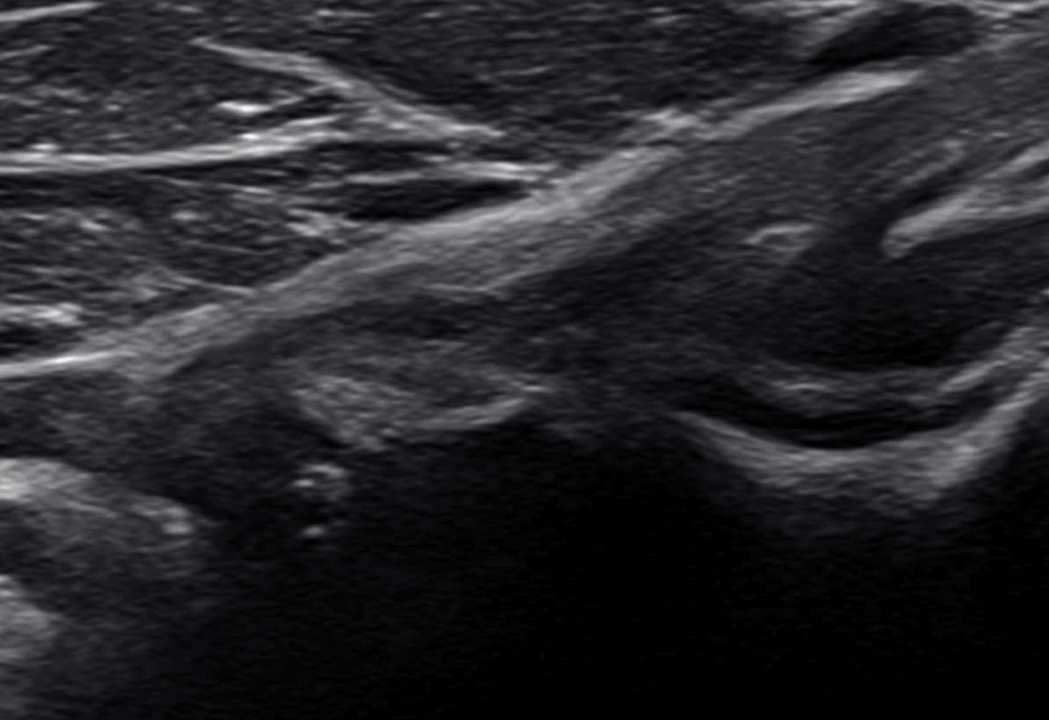
We further examined his thumb joints and the retinaculum of his wrist, and found rhizarthrosis – a form of arthritis – at the first metacarpophalangeal joint. This was an important finding considering the patient’s occupation and physical activities. Its role in the kinetic chain and in fascial restrictions is important for prevention and holistic treatment of the elbow.
There is no perfect modality for radiologic imaging, and some injuries may require a combination of imaging types. However, when it comes to superficial soft tissues and nerves, high resolution ultrasonography has significant advantages over MRI.
Compared to MRI, ultrasonography is clinically friendly, allowing the patient to interact with the doctor to facilitate the diagnostic process. Ultrasound allows for the dynamic examination of joints, muscles, nerves, facia, and ligaments, which is impossible with any other radiologic modality.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















