Our patient is a 33 year-old female who had been suffering from low back pain for 18 years. Three years prior to visiting our clinic, she had developed severe left-sided sciatica. An MRI revealed a spinal anomaly and the patient underwent surgery for a multi-segmental spinal fusion. While the surgery initially relieved her sciatica, she developed new low back pain three years later in the area above the sacroiliac joints, with pain being much worse on the left side.
After the renewed onset of pain, new MRI results were negative and the patient was referred for physical therapy. Despite changing therapists multiple times, physical therapy provided no pain relief. The patient was treated for SI joint instability as a potential pain generator, since her L5-S1 vertebrae were fused. At some point after her surgery she gave birth to a child via C-section. She also suffered multiple sprains without apparent trauma and was diagnosed with Ehlers-Danlos syndrome (EDS).
A physical exam revealed extreme tenderness over both paraspinal surgical scars upon palpation. She was also tender over her C-section scar, and in her gluteal muscles. Her lower abdominal muscles had atrophied from disuse, and her rib cage was scissored and thrusted forward, with multiple fascia densifications along fascia lines.
Ultrasound imaging revealed the following:
Image 1: Normal SI joint and stable ligaments on left side

Image 2: Frayed and tense lumbodorsal fascia, with tenting and traction on the cluneal nerve
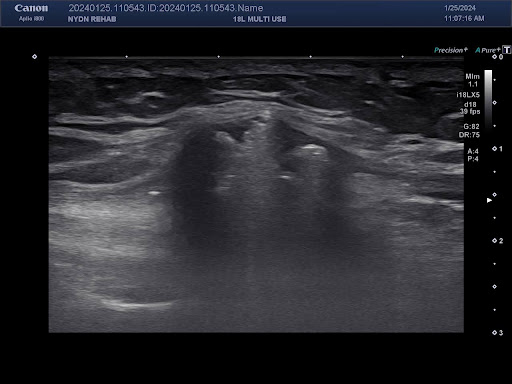
Image 3: R and L comparison of lumbodorsal fascia friction points with spinal hardware (left side has an irregular appearance with sharper edges).

Images 4 and 5: Screws are pinned through the tendinous portion of the paraspinal muscles at their insertion, with more fraying on the left side, and severely thickened and irregular lumbodorsal fascia.
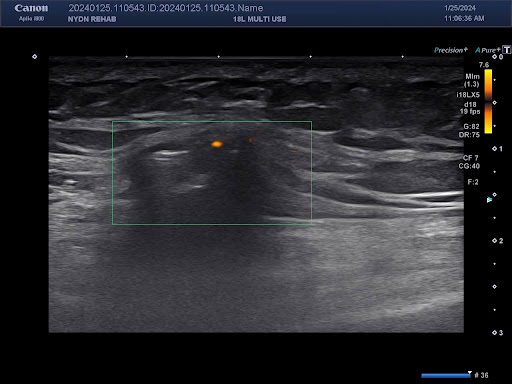
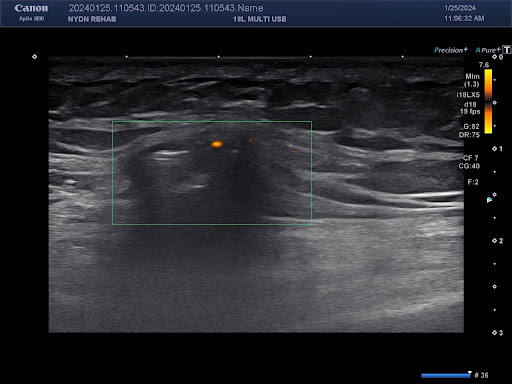
Image 6: Increased doppler signal indicating inflammation over the point of LD fascia contact with hardware.
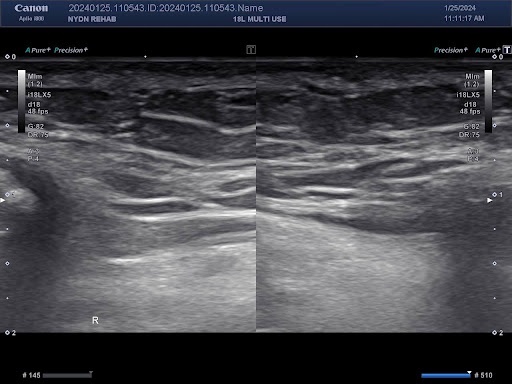
Image 7: Severe atrophy of the multifidus muscles over the fused spinal segments.

The patient is currently being treated under our care, with notable pain relief after just two weeks. Our immediate goals are to restore muscle strength, eliminate pain and inflammation, and treat fascia densifications. Our long-term treatment plan will include physical therapy and other therapeutic interventions to restore functional movement. The patient’s treatment plan will be modified as necessary as we move toward our goals.
This is an example of how surgery for low back pain often not only fails to provide long-term results, but in this case it created more pain and disability for the patient. In most cases, sciatica can be resolved through conservative care and rarely requires surgical intervention. Early intervention could have spared this patient years of pain, and could potentially have spared her a C-section.
In 2022, Dr. Todd Lanman, MD, became the first spine surgeon in the U.S. to reverse a patient’s lumbar spinal fusion and restore full motion by implanting an artificial disc,

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















