Our 41 year-old female patient complained of moderate to severe low back pain. She had gone through five pregnancies – two vaginal and three by C-section. Her back pain commenced about 3 months after abdominoplasty (“tummy tuck”) surgery to correct a 6 cm diastasis recti. The surgery took place 7 months prior to her visit to our clinic.
The patient had originally gone to another practice where an MRI revealed a moderate central L5-S1 protrusion. She was given two epidural steroid injections, followed by three months of physical therapy and acupuncture treatments, with no notable reduction in pain.
We conducted a clinical exam and used a standard Slump test to troubleshoot her lower back pain, and high-resolution diagnostic ultrasound to assess her abdominal region.
We used an intra abdominal pressure stabilization strategy to activate the transverse abdominis and multifidus muscles. Bilateral Slump test results were positive – meaning we were able to reproduce her pain, which we attributed to a shortening of the posterior chain.
Ultrasound imaging of the abdominal wall and low back revealed:
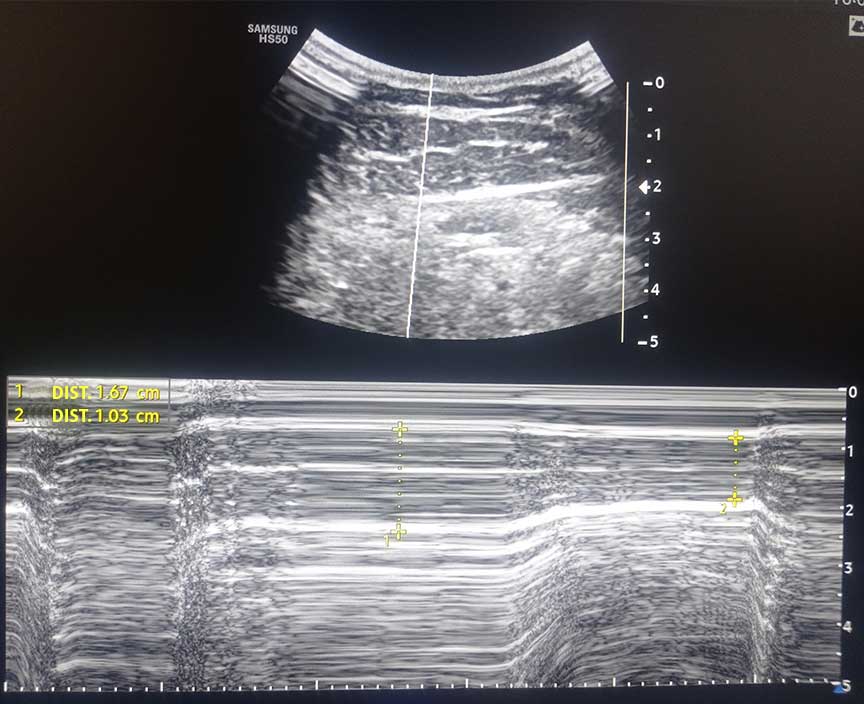
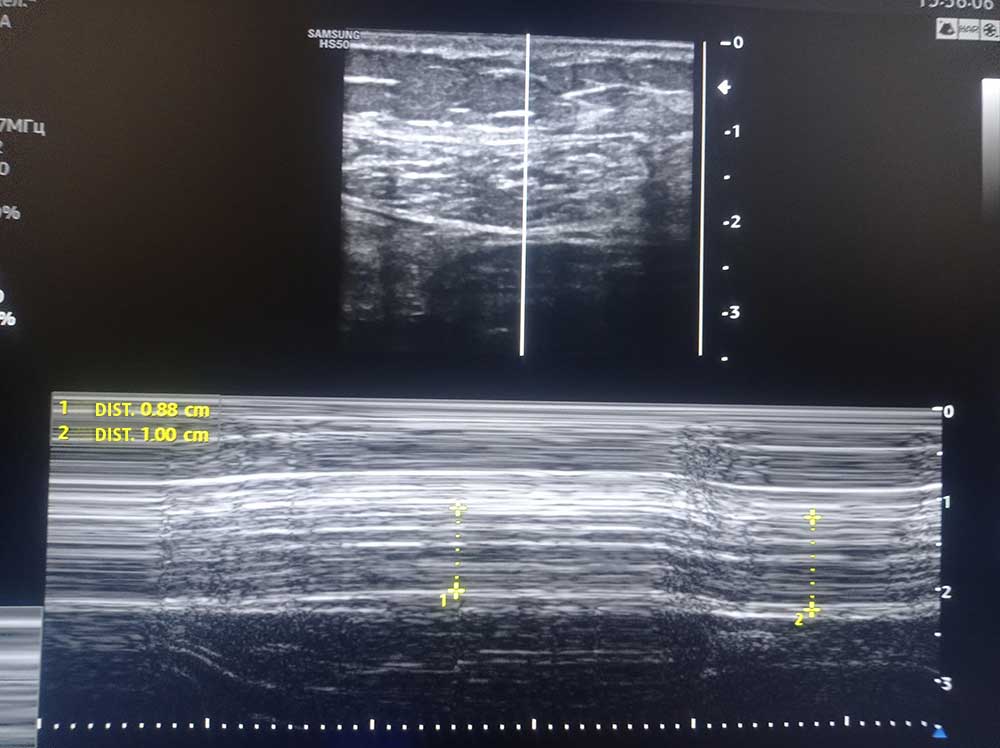

After restoring fascial gliding in the abdomen and the paraspinal muscles, we retrained the activation patterns of the core muscles. With DR-specific physical therapy, we were able to reduce the linea alba gap by a full centimeter. After 6 weeks of treatment, the patient was completely symptom-free.
The use of epidural steroid injections based on MRI reporting of disc pathology is greatly overused, especially in patients who are asymptomatic. Treating the low back while neglecting to do a thorough clinical examination prolonged the patient’s pain and dysfunction.
Our use of diagnostic ultrasonography coupled with an in-depth understanding of the role of fascial tensegrity allowed us to accurately diagnose the patient and treat multiple issues that were the underlying cause of her low back pain.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















