Our patient is a 53 year-old female who came to us complaining of left shoulder/neck pain, elbow pain, and numbness and tingling extending to her fourth and fifth fingers. In the two weeks prior to her visit to our clinic, her elbow pain had begun to intensify.
The patient had previously seen a pain management doctor who prescribed an MRI.
The MRI results revealed:
She was treated with two epidural injections and three months of physical therapy, with no improvement in her condition.
Our clinical exam revealed multiple issues that appeared to be contributing to the patient’s pain and dysfunction:
A Spurling compression test of the cervical spine did not replicate her symptoms. However, she did test positive for the Tinel sign – a pins and needle feeling elicited by tapping on the ulnar nerve at the cubital tunnel. This test reproduced her shoulder pain and mild paresthesia into her fourth and fifth digits.
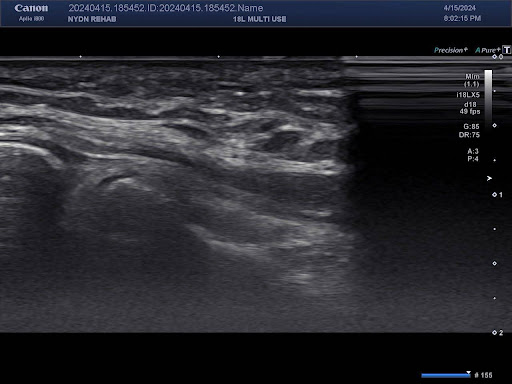
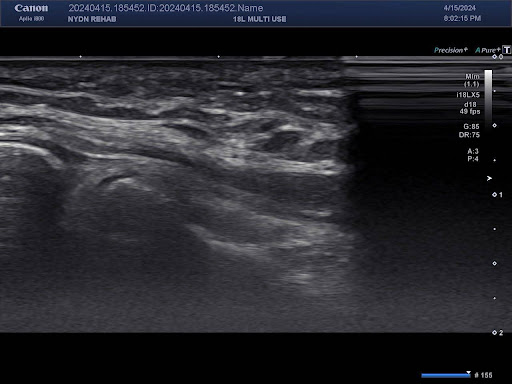
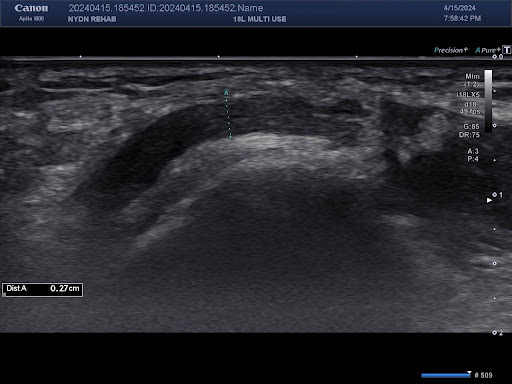
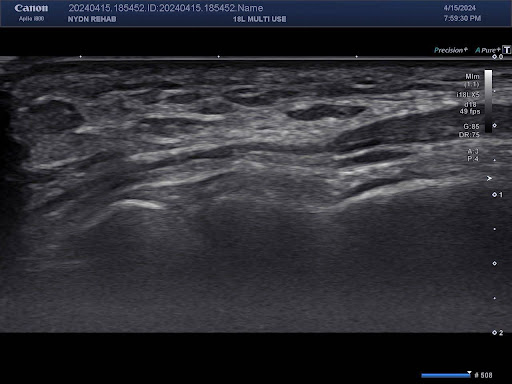
A thorough exam of the affected tissues and structures using high resolution diagnostic ultrasound revealed multiple issues:
Compression and entrapment of peripheral nerves is fairly common and routinely underdiagnosed. Consequently, a neglected subclinical compressed nerve often degenerates into true neuropathy.
Multiple research studies show that nerve compression can create pain due to:
Patients presenting with musculoskeletal pain, especially pain traveling to peripheral nerves, should be examined for nerve compression, both clinically and via high resolution ultrasonography.
Herniated discs in the spine are common and do not always produce pain. However, doctors should be aware of peripheral nerve compression and entrapment, as well as double crush syndrome – peripheral nerve compression at two or more locations along the course of a nerve.
Many doctors, chiropractors and physical therapists do not have access to diagnostic ultrasonography, nor are they sufficiently trained to use it. Most rely solely on magnetic resonance imaging (MRI) to diagnose musculoskeletal pain. However, MRI does not have high enough resolution to detect compressed peripheral nerves, which are extremely common. Consequently, the patient may present with pain in distal from the site of nerve compression, leading to misdiagnosis and ineffective treatment.
A comprehensive knowledge of nerve distribution and muscle innervation, along with advanced clinical examination skills and experience with diagnostic ultrasonography, are all prerequisites for the successful diagnosis and treatment of musculoskeletal pathologies.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination


















