
Posture Optimization
Personalized boutique services supported by cutting-edge integrative diagnostics and advanced holistic therapies.
Meet Posture Specialist Dr. Lev Kalika
Clinical director & DC RMSK
Verified Expert Profiles
Dr. Lev Kalika, DC, RMSK, is a world-recognized expert in integrative rehabilitative medicine, with 20+ years of clinical experience in diagnostic ultrasonography. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. Dr. Kalika is a seasoned biomechanist with an in-depth understanding of human anatomy and musculoskeletal dysfunction.
Dr. Kalika obtained his certification in Posturology under the tutelage of Dr. Bernard Bricot MD, the creator of Total Postural Reprogramming. He studied directly under the world-famous Dr. Vladimir Janda MD, a pioneer in rehabilitative medicine who introduced the concepts of upper- and lower-cross syndrome – key factors in postural misalignment. He is also certified in Dynamic Neuromuscular Stabilization (DNS), an innovative approach to resolving movement disorders, which he learned directly from its founder, Dr. Pavel Kolar.
What is Posture and Why Does It Matter?
Human posture refers to the way the body’s structures align relative to the ground, whether sitting, standing, or in motion. We can liken optimal posture to a finely-tuned machine, where all moving parts are precisely coordinated to interact without friction. When a single part breaks or malfunctions, it can disrupt the mechanical efficiency of the entire apparatus, leading to progressive dysfunction and deterioration.
Unlike a machine, the human body is more than the sum of its parts, and restoring mechanical efficiency requires more than simply swapping out a broken part for a new one. Dysfunction in one area can cause pain and degeneration in another, triggering a cascade of events that reduce mobility and undermine total health.

- Reduced balance and coordination
- Inefficient breathing mechanics
- Poor digestion
- Back and neck pain
- Joint pain and dysfunction
- Reduced athletic and physical performance
- Development of myofascial compensation patterns
In addition to physical dysfunction, poor posture has psychosocial ramifications. The way you carry yourself speaks volumes about your state of mind and sense of self-worth, and poor posture can reinforce negative psychological states. A hunched-over posture is often linked to negative thoughts, moodiness, low self-confidence, and feelings of worthlessness. At the same time, slouching restricts your breathing, elevates stress hormones, and heightens feelings of anxiety and depression.
From an aesthetic perspective, poor posture can alter body proportions, change your facial features, and affect your perceived attractiveness. In the fashion world, poor posture can ruin even the most costly and well-designed couture. Good dynamic posture enhances aesthetics by making movements appear graceful, confident, and athletic.
The following table summarizes how posture influences perception:
| Perception | Upright/Open Posture | Poor/Slouched Posture |
|---|---|---|
Static vs Dynamic Posture
There is more to posture than stationary alignment – it also encompasses the alignment and interaction of body segments during physical activity. Posture plays a key role in your body’s ability to coordinate muscle recruitment patterns and adapt to outside forces. Balanced dynamic posture gives you the ability to keep your body in equilibrium, and to regain balance after body segment alignment is disrupted. When an athlete has good dynamic posture, adaptation is automatic and muscle action is quickly coordinated in real time.
Static posture forms the foundation for dynamic posture, but poor static posture can limit your coordination and adaptability during physical activity and lead to the development of inefficient compensation patterns. Poor body alignment can weaken joint stabilizers and cause imbalances in muscle tension, reducing movement efficiency and increasing your risk of injury.
However, posture is highly trainable, and certain functional exercises and interventions can help to improve both static and dynamic posture over time.


Non-behavioral factors that cause poor posture include:
- Inefficient stabilization system at birth that reduces your ability to defy gravity.
- Neurological dysfunction that diminishes sensory analysis, such as poor eyesight, temporomandibular dysfunction, issues affecting the inner ear, and dysfunctional proprioception in the lower extremities.
- Organ and systemic dysfunction involving respiration, digestion and gastrointestinal issues, dental problems, and gynecological factors that force your posture to adapt in inefficient ways.
- Previous traumatic injuries that cause compensation patterns and disrupt optimal neuromuscular pathways.
- Poor vision that disrupts sensory feedback.
When faced with such issues, your brain automatically favors your vital organs over your musculoskeletal system, creating adaptations that undermine posture and mobility.
Vision and Posture: What's the Connection?
Most postural correction efforts focus on muscle strength and balance, attempting to alter the forces that pull the body into alignment. But that is only a small part of the picture. According to posture specialist Dr. Bernard Bricot, posture is more than a muscle problem – it is a regulatory problem involving brain-managed inputs that work together to keep the body upright, spatially oriented, and ready for movement.
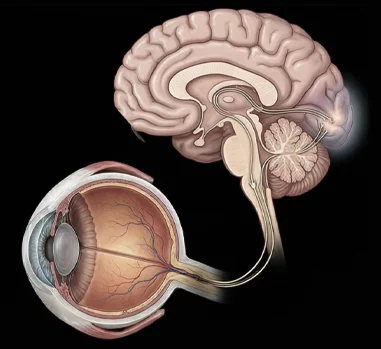
Providing feedback from the eyes and visual processing.
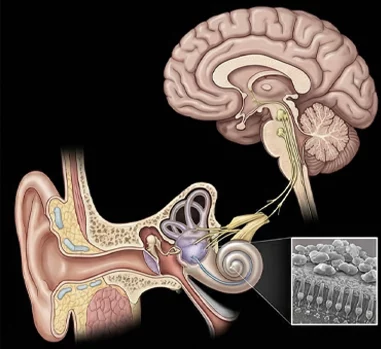
Conveying information from the inner ear for motion and gravity detection.
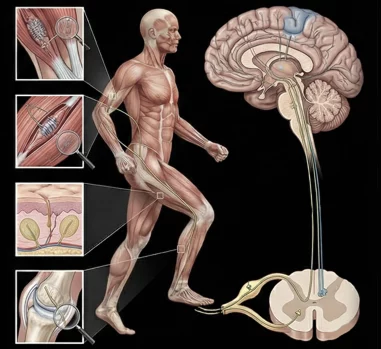
A widespread network of neural receptors, including mechanoreceptors, nociceptors, and proprioceptors. The somatosensory system delivers feedback from proprioceptors in the muscles, fascia, joints, and skin, informing the brain about the body’s spatial position.
Of the three systems, vision accounts for up to 70% of postural control in stable environments. The eyes send constant information to your brain about your body’s spatial orientation, helping to fine-tune muscle activation patterns and fascial tension to maintain optimal stability and alignment.
Your visual system plays a major role in maintaining balance, alignment, and upright posture, but it’s a two-way street – your visual input helps to dictate posture, but poor posture can also affect your visual perception. Good posture relies on synchronicity of the eyes, vestibular system, and neck muscles. If the eyes cannot focus properly, the brain restricts movement, leading to a stiff neck, rigid spine, and poor posture.
Suboptimal visual input due to poor eyesight, poor eye alignment, or inadequate light can undermine visual signaling, reducing the body’s overall stability and balance, and increasing reliance on the vestibular and somatosensory systems. When your visual system fails to provide accurate input, your body may develop compensation patterns that become habitual over time, leading to poor posture.

- Forward-head posture, with craning of the neck and hunching in an effort to bring objects into clearer focus.
- Head tilting due to binocular vision dysfunction, where the eyes do not align, causing double vision or eye strain. Head tilting is a compensation to reduce mismatched signaling.
- Slouching forward, causing posture to defensively collapse when visual processing becomes challenging.
- Frequent shifting of posture, especially during prolonged visual endeavors like reading or focusing on a computer screen that causes visual fatigue.
Such compensation patterns affect the neck, shoulder and back muscles, causing pain, stiffness and headaches. Tight muscles can lead to nerve compression and restricted blood flow. Altered head position can cause eyestrain, blurred vision, and slower visual processing. Chronic head-forward position adds about 10 pounds per inch of load on the cervical spine, disrupting signals between the eyes, brain, and body.
The eyes and oculomotor muscles serve as key posture informants, keeping the central nervous system continually aware of the head’s position in space, and conveying information about the stability of the visual landscape. Convergence of the eyes on a set point is a critical factor. When convergence is insufficient, asymmetrical, or unstable, the nervous system strives to solve the vision problem by reorganizing the body.
The visual system does not provide the only sensory input for maintaining posture, but it plays a substantial role, and vision should be factored into any well-rounded posture optimization protocol.
Fascia, Biotensegrity and Posture
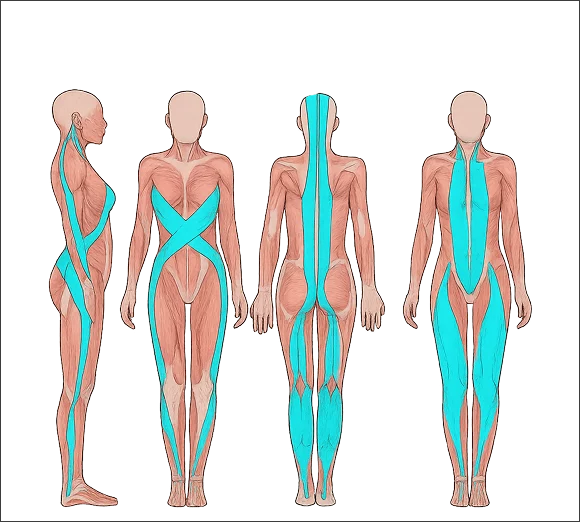
Optimal posture does not happen on its own. Your body’s structures are aligned and held in place by your myofascial system – the network of muscles and fascia that create elastic tension throughout your body – a concept called biotensegrity.
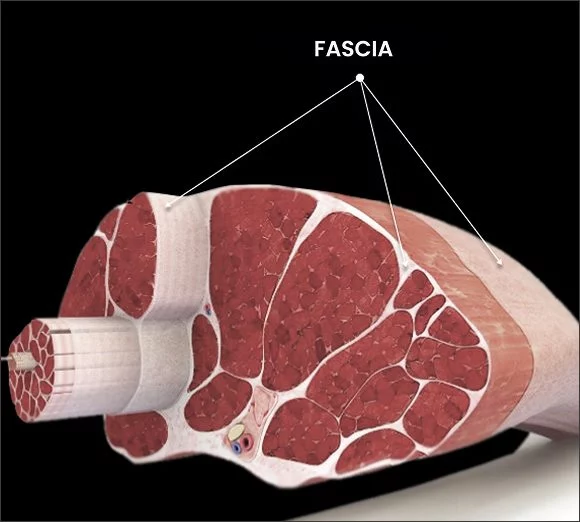
When your muscles contract, they pull against your bones, creating a biomechanical lever system that produces movement. But muscle action and the forces it produces are held in check by fascia, a body-wide network of slippery, elastic connective tissue that helps to control and guide movement, allows for frictionless gliding of the body’s structures, and helps to distribute forces. When muscles and fascial tissues are trained and healthy, movement becomes more precise and efficient, and posture is optimized.
Biotensegrity comes from balanced tension distributed across the entire body, and the position of one body segment influences the position of others. For example, your lower extremities and your ribcage dictate the position of your pelvis, which in turn dictates your spinal alignment. Attempting to fix posture in a single isolated body segment is an exercise in futility, since the position of every segment is affected by – and affects – others.
When damaged by trauma or overuse, or when neglected from lack of use, fascia can become dense and sticky, losing its elastic and lubricating properties.
Fascial densification( adhesions) describe what they are and how they affect posture
Fascial distortions- area of critical connection through which multiple muscle chains converge. These areas are often subject to postural chronic as well as traumatic stress as they are load transfer areas. Dr. Kalika is an expert of diagnostic ultrasonography of fascia and examining these areas is always a part of his exam.
Upper- and Lower-Crossed Syndrome
Upper-Crossed Syndrome (UCS) and Lower-Crossed Syndrome (LCS) are concepts introduced by renowned Czech physician Vladimir Janda. Dr. Kalika received early training directly from Dr. Janda, laying the groundwork for his career in integrative medicine.
The syndromes describe common patterns of muscle imbalances caused by factors such as poor posture, prolonged sitting, inactivity, and asymmetrical repetitive movements. As a result, some muscles become too tight while others become too lax, creating instability and forming a “crossed” pattern of dysfunction.
Both syndromes often stem from modern lifestyles: sedentary behavior, poor ergonomics, stress, lack of movement variety, or repetitive forward-leaning activities. UCS is more common with upper-body-dominant habits, while LCS ties to sitting or weak core/glutes.
Upper Crossed Syndrome (UCS)
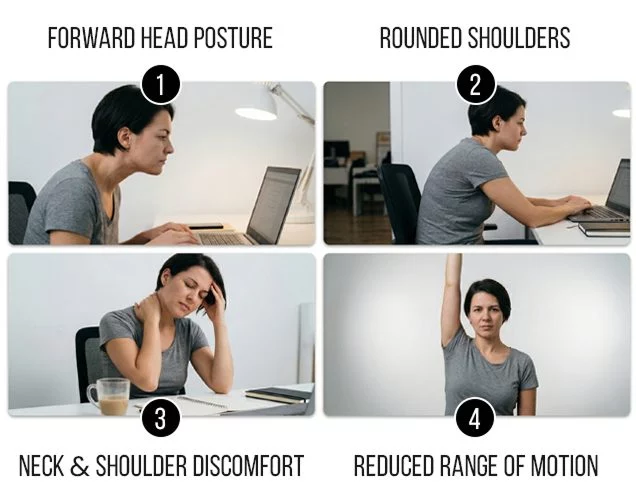
The upper cross affects the trunk, neck, shoulders and upper back. It encompasses a chronic head-forward posture that is increasingly seen with the use of technological devices.
UCS is marked by changes such as:
- Forward head posture
- Rounded shoulders
- Thoracic kyphosis (hunched upper back)
- Neck and upper back pain
- Frequent headaches
- Shoulder discomfort
- Reduced range of motion
Upper Crossed Syndrome affects multiple muscles:
| Category | Muscles | Status | Typical Role in the Pattern |
|---|---|---|---|
| Tight / Overactive | Upper Trapezius | Tight | Elevates shoulders, contributes to shrugging |
| Tight / Overactive | Levator Scapulae | Tight | Elevates scapula |
| Tight / Overactive | Sternocleidomastoid (SCM) | Tight | Forward head pull |
| Tight / Overactive | Pectoralis Major & Minor | Tight | Rounds shoulders forward |
| Tight / Overactive | Suboccipitals | Tight | Extends upper cervical spine |
| Lax / Underactive | Deep Neck Flexors | Weak / Lax | Opposes forward head posture |
| Lax / Underactive | Middle & Lower Trapezius | Weak / Lax | Retracts & depresses scapula |
| Lax / Underactive | Rhomboids | Weak / Lax | Retracts scapula |
| Lax / Underactive | Serratus Anterior | Weak / Lax | Protracts & stabilizes scapula |
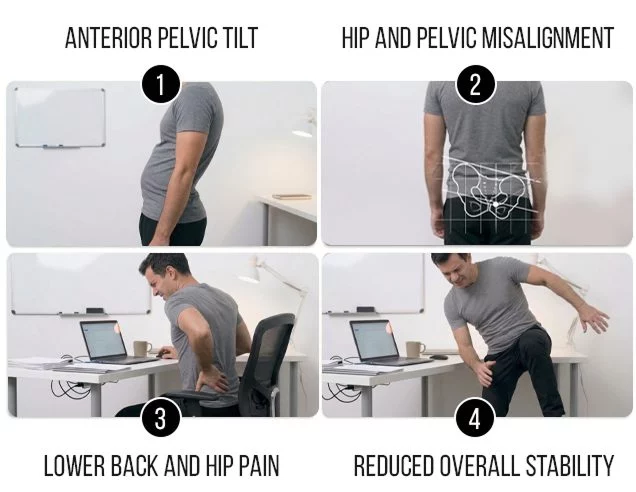
Lower Crossed Syndrome (LCS)
LCS affects the muscles and joints of the lower body, from the hips and pelvis to the feet. It is typically linked to prolonged sitting and lack of physical inactivity.
Postural changes linked to LCS include:
- Anterior pelvic tilt
- Increased lumbar lordosis
- Hip and pelvic misalignment
- Spinal misalignment
- Lower back and hip pain
- Reduced overall stability
Lower crossed syndrome affects the following muscles:
| Category | Muscles | Status | Typical Role in the Pattern |
|---|---|---|---|
| Tight / Overactive | Iliopsoas (Hip Flexors) | Tight | Anterior pelvic tilt |
| Tight / Overactive | Rectus Femoris | Tight | Assists hip flexion |
| Tight / Overactive | Erector Spinae (Lumbar Extensors) | Tight | Increases lumbar lordosis |
| Tight / Overactive | Quadratus Lumborum | Tight | Assists lumbar extension & side bending |
| Tight / Overactive | Tensor Fasciae Latae (TFL) | Often Tight | Contributes to tilt & IT band issues |
| Lax / Underactive | Abdominals (Transversus Abdominis, Internal/External Obliques, Rectus Abdominis) | Weak / Lax | Core stability, opposes anterior tilt |
| Lax / Underactive | Gluteus Maximus | Weak / Lax | Hip extension, posterior pelvic control |
| Lax / Underactive | Gluteus Medius & Minimus | Weak / Lax | Hip abduction & stabilization |
Diagnostic Tools for Assessing Posture
Posture assessment can be challenging due to the fact that each person has a unique anatomy, and every body is used in ways unique to its owner and lifestyle. Postural assessment typically combines subjective observational factors with more objective tools to identify alignment issues, quantify deviations, and guide treatment.
Common assessment tools include:
- Visual assessment from the anterior, posterior and lateral viewpoint.
- Plumbline assessment that looks for alignment of key sites, such as the ear, shoulder, hip, knee and ankle.
- Wall grid assessment, where the clinician looks for deviations as the patient stands in front of a wall-mounted grid.
- Goniometer assessment of joint angles, to identify postural markers like head-forward, shoulder protraction, or anterior pelvic tilt.
- Digital inclinometer, to measure exaggerated spinal curvatures.
- Photographic analysis.
At NYDNRehab, we use advanced tools to assess both static and dynamic posture. Our high-tech lab pairs advanced technologies with proprietary software to give us quantitative data about your body alignment, at rest and in motion. We use that information to create a posture retraining program and a baseline for measuring progress.

Your posture assessment at NYDNRehab may include:

Head-to-toe evaluation using high-resolution ultrasonography, to look for anomalies that contribute to postural deviation.

3D biomechanical analysis to assess movement patterns, joint angles, mass distribution, and other key factors.

3D gait analysis to identify mechanical gait deficits.


Task-specific dynamic tests.
Posture Optimization Training
Postural optimization involves reprogramming the brain, nervous system, and muscles to correct, improve, and maintain optimal structural alignment. The goal is to build long-term muscle memory through specific exercises, movement retraining, and increased body awareness. The reprogramming process counteracts poor postural habits like rounded shoulders and exaggerated pelvic tilt.
Once we have a clear and comprehensive picture of the factors affecting your posture, we create a customized posture retraining protocol based on your results.

- Dynamic Neuromuscular Stabilization (DNS) to activate innate developmental motor strategies.
- Fascial manipulation and trigger point therapy to restore the elastic and gliding properties of densified fascia.
- Rehabilitation of old injuries that are causing compensation patterns.
- Neuromuscular feedback training to restore coordinated muscle activation patterns.
- Strengthening and stretching exercises to promote stability and restore balanced muscle tension.
- Patient education, to help you maintain your posture optimization results.
Tips for Achieving and Maintaining Optimal Posture
Poor posture is often habitual, formed by years of inefficient motor strategies, repetitive overuse, and suboptimal workplace ergonomics. Adopt the following strategies to gradually improve your posture and maintain it over time.
- Set posture reminders at 30-60 minute intervals to check and reset your posture. Arrange your ears over your shoulders, relax your neck and shoulders, align your head over your spine, tuck your chin slightly, and neutralize your pelvis.
- Optimize your work station ergonomics. Place your computer screen at eye level, make sure your chair supports your natural lumbar curve, and keep your feet flat on the floor. Get up and move every 30 minutes if desk-bound.
- Avoid prolonged sitting and slouching. Stand up to take phone calls, and use a standing desk if possible.
- When standing or walking, gaze straight ahead, contract your core, lift your chest, and pull your shoulders back and down.
- Optimize your sleep position by using pillows to support neutral alignment of your neck and spine.
- Practice deep diaphragmatic breathing to engage your core and reduce constriction of your upper chest and neck.
- Do cross-training activities to offset asymmetrical movement patterns in sports like golf, lacrosse and baseball.
- Get regular exercise that targets all your major muscle groups, and be sure to stretch tight muscles and joints.


Real Patient Cases Treated at NYDNRehab
These case studies reflect real clinical conditions evaluated at NYDNRehab using advanced diagnostic methods and individualized rehabilitation strategies. All cases are evaluated and managed by Dr. Lev Kalika and the NYDNRehab clinical team.
Range of Available Unique Physical Therapy
Treatments at Nydnrehab
Certificates and Continuing Education
























Posture Optimization FAQs
Optimal posture maintains the spine’s natural curves, and positions the joints in alignment. It evenly distributes your body mass and minimizes strain on body structures.
While there is no universally “perfect” posture, you can optimize your posture based on your unique anatomical characteristics and daily habits and activities. Good posture spares energy, optimizes movement, and reduces excess strain on individual body structures.
In most cases, posture can be optimized over time through awareness, targeted exercises, ergonomic changes, and consistent habits. However, it is important to distinguish between functional and structural posture deviations. Functional posture is caused by habits, muscle imbalances, poor ergonomics, leg length discrepancies, and compensation patterns, and is typically modifiable. By contrast, structural posture involves permanent or semi-permanent changes to bones, joints, ligaments, or soft tissues. Structural changes often form after a lifetime of wear-and-tear, and can be difficult to correct.
You can do a simple self-assessment of your posture by taking a photo of your reflection in the mirror from the front, side and back, and by assessing pain and discomfort.
Look for:
- Forward head position, with ears ahead of shoulders.
- Rounded shoulders or hunched upper back.
- Excessive lower back arch or protruding abdomen.
- Pain or fatigue in neck, shoulders, back, or hips.
- Difficulty maintaining neutral posture during movement.
- A plumb line that passes from your ear, through your shoulder, hip, knee,and ankle.
Another simple test is to stand against a flat wall with your heels, buttocks, shoulder blades, and the back of your skull touching the wall. Hold that posture and step away from the wall – if it feels unnatural, you may need posture correction.
- Heighten your awareness when standing, sitting and moving. Set your gaze straight ahead, engage your core, and pull your shoulders back and down.
- Take frequent breaks from long bouts of sitting to walk, stretch and move around.
- Engage in regular exercise. Daily walking with 2-3 sessions of whole-body resistance training, along with regular stretching, can help you achieve and maintain better posture.
There is no set protocol for optimizing posture, and the pace of improvement varies from one person to the next. Age, adherence, and the severity of postural deviations all factor in. However, a consistent posture optimization program should produce results within several weeks. Consistency is key for any physical training program.
 Lev Kalika
Lev Kalika  Rostyslav Bubnov
Rostyslav Bubnov 




















