Physiotherapists need to pay attention to the demographics of each patient when pain is present in the hips or groin. Age, gender, and activity level are key factors one should consider in diagnosis, as is the speed of onset. If the pain appears to be a result of an injury, the physiotherapist should ask the patient if he or she can supply any remembrance of how, precisely, the injury occurred. If the patient was playing sports, which sport was he playing? Did the injury happen outdoors? Did she remember turning suddenly at a sharp angle? Did he hear a popping sound, or feel something tearing? Does she feel something catching while she tries to walk? Palpate the entire area carefully and gently, and always respectfully, remembering that the patient and any direct observations are your primary resources for information.
If the patient reports a soccer or football injury, that is, kicking while running, suspect a flexor tear. The patient will feel pain upon lifting the leg upward, stretching the flexor muscle, or suspending in that position. Compare to the non-injured side as well if possible. These tears can also runners, particularly sprinters.
An adductor tear occurs when kicking hard, or sudden, unexpected, or forceful use of that muscle occurs. This can happen on an unlit staircase or a sidewalk edge. Palpate the area firmly but carefully, or try stretching it to see if the patient reports increased pain.
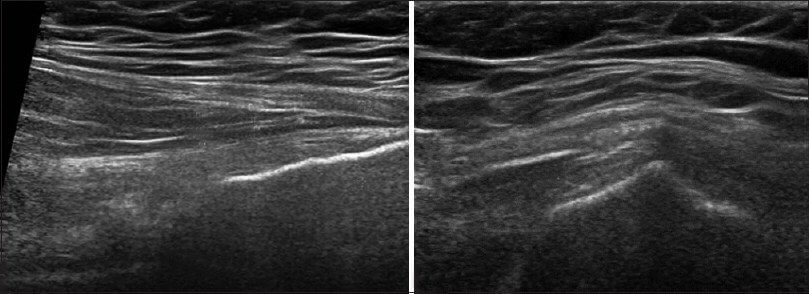
A labral tear is not a cartilage tear per se but damage to the lining of the cartilage in the hip socket. The patient will report a clicking sensation or perhaps a feeling that something is catching while he is walking. The pain is deep inside or within the groin, but could be referred as vague groin pain. Patients usually report increased pain while weight-bearing or walking.
Sometimes, hip or groin pain is referred from elsewhere, such as the lower back. Often this might present as a “pins and needles” sensation or numb feeling.
Rarely, physiotherapists may encounter pain that is referred from another area, but in fact, is felt in the groin. Often, the source is in the lower back, but always check the patient’s footwear, and the condition of the knees and lower legs as well.
With elderly patients, postmenopausal women especially, osteoarthritis can be a factor in hip pain. The onset is usually gradual. Elderly patients with poor bone density need to learn to strengthen their muscles to avoid any falls in the future.
Almost always, a fractured hip is so painful that the patient cannot bear weight nor walk on her own. Since dementia may also complicate matters, this type of injury is often rather stressful for families and patients alike.
Physiotherapists should be culturally aware and realize that not all patients express pain the same way. Pay careful attention to athletic concerns and the particularities of the sport and movements involved. Athletes may have concerns about how soon they can return to full functioning. Be sure to understand what this means, as for each patient, functionality is an individual matter that must be respected.