Complex regional pain syndrome (CRPS) is a painful and sometimes debilitating neuro-inflammatory disorder that arises after a minor traumatic limb injury such as a sprain, strain, fracture or scrape, or sometimes after surgery or immobilization. Previously referred to as reflex sympathetic dystrophy (RSD), the condition affects roughly 80,000 Americans each year. The syndrome is marked by increased pain over time that is more severe than one would expect from the original injury.
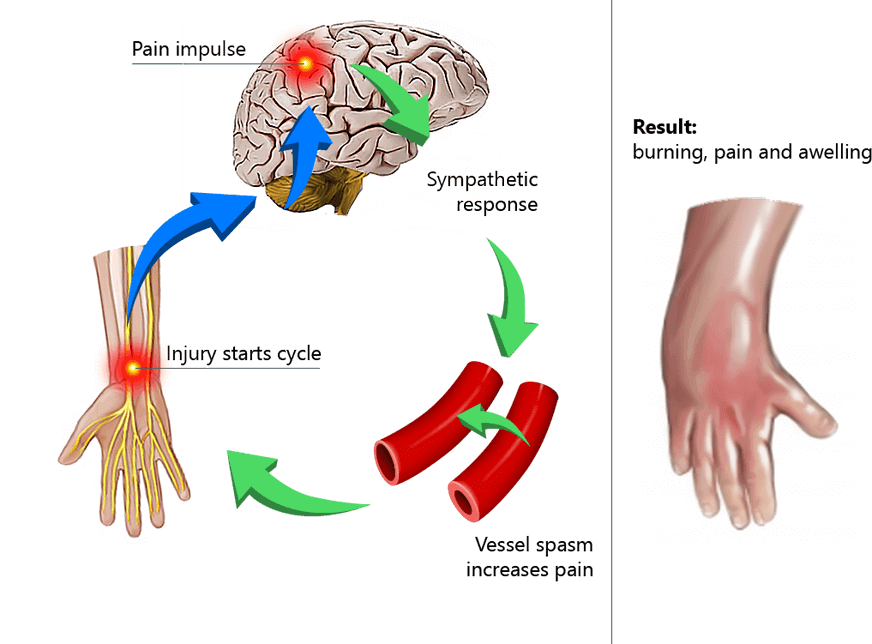
CRPS is caused by a malfunction of the nervous and immune systems in response to tissue damage from trauma, causing nerves to misfire and send constant pain signals to the brain. CPRS normally affects an injured limb, but can also occur in the hands, feet, or back. The most common occurrence of CRPS is after a fracture to the distal radius, at the thumb side of the wrist.
CPRS can be divided into two subcategories:While CRPS can affect anyone at any age, it most commonly affects people in their mid 30s, with females 3.5 times more likely to report the condition than males.
The main symptom of CRPS is pain that increases after an injury, rather than decreasing as the injury heals. Other symptoms may include:
There is no single or simple diagnostic tool for CRPS. Diagnosis is mostly based on patient history, clinical examination, and laboratory results. Other conditions that might be the source of pain must be ruled out before considering a diagnosis of CRPS.
Early diagnosis and treatment are important for resolving CRPS.
Conventional treatments for CRPS revolve around pain management, and most involve some type of pharmaceutical intervention. Common treatment approaches include:
It is important to note that conventional methods of treating CRPS are focused on managing the symptoms, rather than resolving the condition. Moreover, any type of cold therapy should be avoided, as it can accelerate the disease and worsen symptoms.
At NYDNRehab, we take a holistic approach to CRPS treatment, paying close attention to the unique needs of the individual patient. Physical therapy treatment is geared to increasing strength and mobility while gradually reducing and eliminating pain and other symptoms.
At NYDNRehab we mainly concentrate on:
Progressive desensitization techniques to stimulate and desensitize the painful area.
We also use our C.A.R.E.N system for pain modulationand cortical integration.
The end goal of treatment is to improve strength and range of motion while reducing the perception of pain, helping the patient achieve more normal function without pain.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































