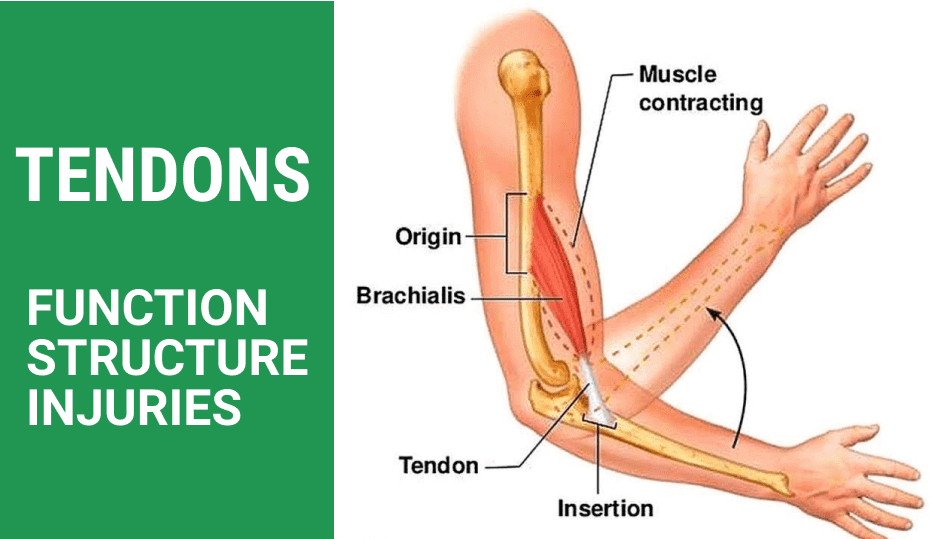
Tendon injuries are common among athletes, runners and other physically active populations because of the fundamental role they play in human movement. Tendons are a type of connective tissue that is continuous with muscle tissue, anchoring muscles to boney structures to produce movement. When the muscle contracts, or shortens, the tendon pulls against its boney attachment, causing it to rotate around the associated joint.
During physical activity, the tendinous portion of the muscle-tendon unit is subjected to large force loads, making it vulnerable to injury. Depending on the type, intensity and duration of activity, various tendons throughout the body are called upon to overcome opposing forces many times the athlete’s body mass. For example, running, jumping and landing can generate peak force loads of up to 12.5 times body weight.
For decades, steroid injections have been liberally used to treat tendinopathy, providing short-term pain relief and reducing inflammation. But a growing body of research indicates that steroid injections may actually do more harm than good in the long run.
Tendons are strong fibrous bands of connective tissue that attach muscles to bones. Their structure relies the interplay of local cells and the extracellular matrix (ECM), made up of parallel collagen fibers. The fibers are bundled and surrounded by layers of connective tissue that minimize friction during movement and supply deep tendon structures with blood vessels, nerves, and lymphatics. It was recently discovered that tendon tissue contains tendon stem/progenitor cells (TSPCs), with properties common to other types of stem cells.
Because tendons are stiffer than muscles, they possess greater tensile strength and are able to withstand large force loads without deforming, enhancing the ability of muscles to transmit forces to the bones without expending energy to stretch the tendons. Beyond transmitting forces from muscle to bone, tendons store elastic energy, contributing to force production during intense physical activity.
Tendinopathy occurs when force loads are greater or more frequent than the tendon is able to adapt to. Ideally, overloading the muscles and tendons stimulates the cells to become denser and stronger. But when there is insufficient recovery time, the tissue begins to break down, progressing through four phases that eventually lead to cell death and tendon ruptures:
Phase 1: Reactive Tendinopathy: This is the normal post-exercise phase where adaptation takes place, provided the tendon is given ample time to recover.
Phase 2: Tendon Disrepair: In this phase, the rate of injury exceeds the rate of repair.
Phase 3: Degenerative Tendinopathy: Tendon cells begin to die.
Phase 4: Tendon Rupture: Tendon tissue breaks down, leading to tendon tears and loss of function.
During phases one and two, the tendon is still able to repair itself. In phases three and four, medical intervention is required to rehabilitate the tendon. Torn or ruptured tendons can take months to fully heal. In some cases, tendon ruptures cause permanent disability.
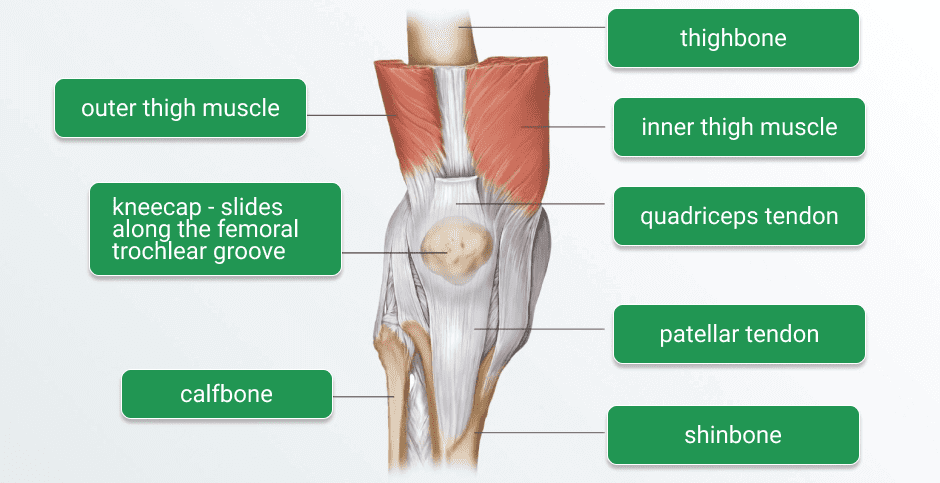
Repetitive overuse is the primary underlying cause of tendinopathy. In runners, for example, up to 75 percent of injuries are attributed to overuse, most of which affect the Achilles tendon and the tendons surrounding the knee.
The most common sites of tendinopathies and the activities that cause them include:
Achilles tendon (ankle): Soccer, tennis, volleyball, diving, basketball, running, gymnastics, dance, cycling
Patellar tendon (knee): basketball, volleyball, soccer, football, track, tennis, dance, gymnastics and skiing
Hamstring tendons (biceps femoris, semitendinosus, semimembranosus): Football, soccer, tennis, basketball, and field sports involving sprinting, cutting and sudden stops and starts
Rotator cuff tendons (shoulder): Swimming, rowing, tennis, baseball, weight lifting
Lateral epicondyle (elbow): Tennis and other racquet sports
Medial epicondyle (elbow): Golf, baseball, javelin and other throwing sports
Since their initial debut in 1948, corticosteroid injections for musculoskeletal pain have become widespread. Steroid hormones bind to glucocorticoid receptors found in every human cell, providing short-term pain relief. However, there is no evidence that corticosteroid injections provide long-term benefits, and growing evidence that they may have negative long-term effects on tendon cells.
Recent research reveals that local steroid injections reduce tendon cell viability and proliferation, and undermine collagen synthesis. Collagen in the tendon becomes disorganized and cells begin to die, significantly reducing the tendon’s mechanical properties. Despite their ability to provide temporary pain relief, it is increasingly clear that steroid injections are harmful to tendons in the long run, weakening them and making them more susceptible to injury.
Tendinopathy rehabilitation requires accurate diagnosis and complex clinical reasoning. The location and degree of damage must be accurately assessed, taking into account the patient’s activity status, functional assessment, and any other co-existing issues along the kinetic chain.
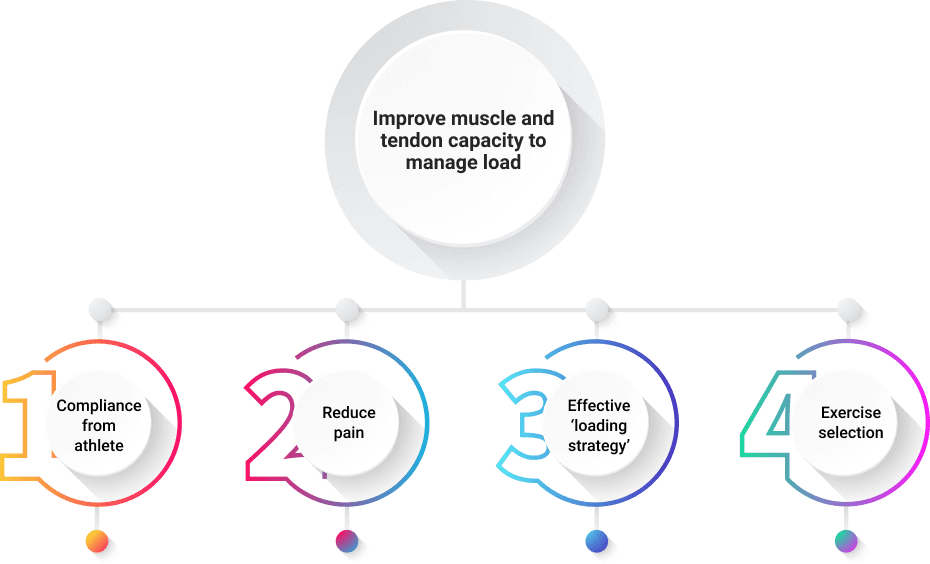
There is a general consensus that rest is not an effective treatment option for tendinopathy. The primary goal of rehab is to increase the capacity of the muscle-tendon unit to manage load. Essential co-factors are patient compliance, pain management, exercise selection and a carefully designed loading strategy.
The sports medicine specialists at NYDNRehab work with hundreds of athletes to rehabilitate injuries, correct mechanical deficiencies and enhance performance. We use advanced technologies and innovative treatment methods not found in most rehab clinics.
Some of our clinical tools for treating tendinopathy include:
Don’t let tendinopathy take you out of the game. Contact NYDNRehab today, and get the best sports medicine physical therapy in NYC, so you can safely return to play.
Resources
Cardoso, Tanusha B., et al. “Current trends in tendinopathy management.” Best Practice & Research Clinical Rheumatology (2019).
Dean, Benjamin John Floyd, et al. “The risks and benefits of glucocorticoid treatment for tendinopathy: a systematic review of the effects of local glucocorticoid on tendon.” Seminars in arthritis and rheumatism. Vol. 43. No. 4. WB Saunders, 2014.
Lipman, Kelsey, et al. “Tendinopathy: injury, repair, and current exploration.” Drug design, development and therapy 12 (2018): 591.
Wu, Fan, Michael Nerlich, and Denitsa Docheva. “Tendon injuries: basic science and new repair proposals.” EFORT open reviews 2.7 (2017): 332-342.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































