HomeBlogESWT Treatment for Chronic Lateral Epicondylitis Study Recap
ESWT Treatment for Chronic Lateral Epicondylitis Study Recap
Can ESWT Treat Chronic Lateral Epicondylitis Effectively? A Major Study Says Yes.
Chronic lateral epicondylitis (CLE) is the formal name of a condition that many people call tennis elbow. If you suffer from this ailment, the outer part of your elbow is often tender or in pain, and that discomfort increases when you perform actions that exert your wrist, including opening a jar, brushing your teeth, shaking someone’s hand, and lifting objects.
When you repeatedly use the tendons and muscles of your forearm, in the same way, it can lead to CLE. Half of all regular tennis players acquire it, and many golfers, gardeners, and carpenters do as well. In fact, 16 percent of the people who file for workers’ compensation have CLE.
What Is ESWT?
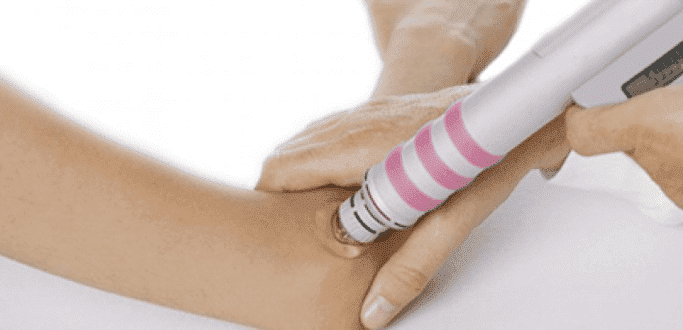
Extracorporeal shockwave therapy (ESWT) is emerging as a promising way to treat CLE. When patients undergo ESWT treatment, they’re fitted with a pad and administered shockwaves, which are quick, pulsating bursts of energy. Those waves pass from the pad through the skin.
A major medical study suggests that a single session of intense ESWT can be efficient at remedying CLE. In many cases, patients can go back to their jobs within a week after this therapy, which is much sooner than if they’d had surgery.
However, for about three weeks after patients receive this treatment, they aren’t supposed toms are diminishing.
People often experience further improvements after three months, six months, and a year, which is the typical pattern for a tendinopathy that’s healing.
As their conditions improve and after they consult with their docto playing sports.
ESWT’s Roles-Maudsley Scores
The American Journal of Orthopedics published the results of a medical study that quantified the success rates of ESWT treatment in dealing with CLE. In part, it did so by using the Roles-Maudsley system of scoring. It calls for participants to 4.
Obviously, these measurements are subjective and depend on each patient’s tolerance for pain, but they can provide researchers with an overall sense of how well a certain type of therapy works. The numbers translate as follows:
1 is excellent. There’s no pain whatsoever. 2 is good. There are bouts of discomfort here and there, but a person has no restrictions as far as activities and lifestyle. 3 is fair. After a person has been active for an extended period, discomfort occurs. 4 is poor. A patient is experiencing regular pain, limiting what he or she can do on a daily basis.
After four weeks, 69.5 percent of patients recorded a score of excellent or good; 19.4 percent rated their condition as fair, and 11.1 percent as poor. Moreover, not one patient reported feeling worse after the treatment than before.
After 12 weeks, 78 percent of the subjects said that their condition was excellent or good; 11.1 percent described it as fair, and 11.1 percent called it poor.
The Study’s VAS Results
In addition, the study measured patients’ rehabilitation using visual analogue scale (VAS) scores. In this system, people rate their pain from 1 to 10; 1 indicates no pain, and 10 describes excruciating pain.
Prior to 2.5.
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating the full thickness tear and already occurring muscle atrophy due to misdiagnosis and not referring the patient to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed to be a complete tear with muscle contraction under diagnostic sonography (not possible with MRI)
Complete tear of rectus femoris with large hematoma (blood)
Separation of muscle ends due to tear elicited on dynamic sonography examination