February 26, 2026

The feet play a foundational role in every sport or physical activity, acting as critical stabilizers and contributing to upward and forward propulsion. Even swimmers use their feet as propellers and rudders, translating force from powerful kicks and ankle motion into forward momentum.
The plantar fascia is a key structure that gives the human foot its remarkable ability to support the body’s mass and contribute to force production. Plantar fasciitis is a condition where repetitive overuse leads to overstretching and micro tears in the plantar fascia, causing pain and limiting its mechanical properties.
Learn about the structure and function of the plantar fascia, new therapies for plantar fasciitis treatment, and how high-load strength training helps athletes to quickly recover from plantar fasciitis.
Fascia is a collagenous type of connective tissue that forms a broad network throughout the human body, encasing and connecting soft tissues, holding organs in place, and working with muscle to guide, control, and translate forces. Fascia’s key properties are tensile strength and elasticity, creating a body-wide system of compression called biotensegrity.
Fascia is richly embedded with hyaluronic acid infused with water molecules, creating a slippery gel that enables tissues, nerves and blood vessels to glide among one another without friction. It is also richly embedded with sensory nerves, making fascia a key pain generator. When damaged, fascia loses its elastic and gliding properties, sending strong pain signals to the brain.

The plantar fascia is a specialized form of deep fascia, made up of densely packed, longitudinally-oriented collagen fibers, that spans the bottom of the foot from heel to toe.
The plantar fascia supports the foot’s longitudinal arch and provides protection for the foot’s nerves, blood vessels and small muscles from compressive forces. It provides stability by preventing excessive foot motion, and absorbs shock from ground reaction forces.
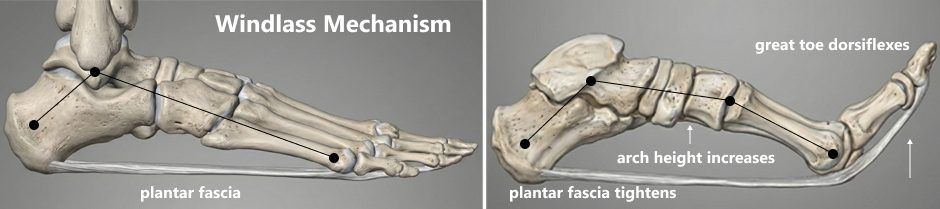
During locomotion and propulsion, the plantar fascia is not a passive structure – it is a key player in activities like walking, running and jumping. At the toe-off phase of the gait cycle, the plantar fascia stores energy as it shortens, creating a rigid lever for propulsion. As the ankle plantar-flexes, forces generated from the legs are translated to the foot, and the plantar fascia lengthens and releases its stored energy, contributing significantly to propulsion – a mechanical action known as the Windlass Mechanism.
Technically, the term “plantar fasciitis” is a misnomer, since the suffix “itis” refers to inflammation. A more appropriate terminology is plantar fasciopathy, because the condition is more degenerative than inflammatory. Plantar fasciopathy is one of the most common overuse injuries in athletes, especially among those in repetitive high-impact sports that involve running, jumping, and landing. The condition accounts for up to 8% of all running-related injuries.
In athletes, plantar fasciopathy is triggered by:
Over time, repetitive overuse causes microtears and thickening of the plantar fascia, causing pain and reducing its capacity for elastic recoil. Pain is often felt most intensely at the origin of the plantar fascia where it attaches to the calcaneus (heel bone). The symptoms of plantar fasciopathy mimic those of other overuse syndromes, making it difficult for clinicians to differentiate plantar fasciitis from bone spurs, calcaneal fractures, or Achilles tendinopathy.
Characteristics of athletic plantar fasciopathy include:






Plantar fasciopathy typically self-resolves over time, and conventional treatment is generally conservative in nature. In 2023, the American Physical Therapy Association (APTA) updated its guidelines for the conservative treatment of plantar fasciitis.
Recommended evidence-based APTA guidelines include:
Other conservative approaches include rest and activity modification, icing/cryotherapy, NSAIDs, corticosteroid injections, and exercises for the intrinsic foot muscles.
Even with the best conservative care, plantar fasciitis can take months or even years to fully resolve. In fact, some experts suspect that by taking a conventional conservative approach, clinicians may be prolonging recovery, leaving patients to deal with pain and disability for months on end. Considering that the condition typically self-resolves over time, patients may question whether medical treatment is making any difference at all.
Thankfully, new advanced treatment approaches are dramatically accelerating the healing process and eliminating pain and dysfunction in a matter of weeks.
In the 21st Century, high costs, overuse of pharmaceuticals, unnecessary treatments and surgeries, and substandard patient outcomes have undermined public trust in conventional medicine. Consequently, more and more, patients are turning to holistic and integrative practitioners for drug- and surgery-free solutions.
At the same time, recent advancements in energy technologies and orthobiologics are equipping holistic practitioners with new evidence-based tools that promote healing and help to restore function, without drugs or invasive procedures. When used proactively in the early stages of plantar fasciopathy, such interventions can help to dramatically shorten recovery time.
Focal Extracorporeal Shockwave Therapy (fESWT)
Shockwave therapy uses high frequency sound waves to reduce pain and inflammation, and to stimulate tissue healing at the cellular level. fESWT is especially effective for treating fibrocartilaginous structures like the plantar fascia, helping to reorganize collagen fibers and stimulate neovascularization.
A 2024 review of randomized control trials involving 1121 patients compared corticosteroid injections – a conventional medical treatment for plantar fasciitis – to shockwave therapy. The researchers found that extracorporeal shock waves outperformed corticosteroids in relieving pain, reducing the density of the plantar fascia, and enhancing foot function.
Ultrasound Guided Dry Needling
Dry needling targets myofascial trigger points – tiny hard nodules of tightly contracted fibers that cause pain and interfere with muscle action. The procedure involves insertion of filament-thin, non-medicated needles through the skin to irritate the trigger point, evoking a twitch response that immediately relaxes the fibers. Ultrasound guidance ensures accuracy, meaning fewer insertions and less discomfort for the patient.
A 2024 systematic review and meta-analysis involving 781 patients found that dry needling combined with conventional methods was more effective than conventional treatments alone in relieving pain and restoring foot function in patients with plantar fasciitis.
Fascial Layer and Nerve Hydrodissection
When fascia is damaged, it becomes dense and sticky, often trapping nerves and blood vessels and preventing them from gliding. During the fascial hydrodissection procedure, a neutral solution is injected between fascial layers, causing them to separate, releasing trapped nerves, and restoring fascia’s ability to glide.
A 2023 review of scientific literature affirmed that ultrasound guided hydrodissection of peripheral nerve entrapments is a useful and efficacious approach that can significantly improve quality of life and, in many cases, prevent the need for surgery.





Myofascial release is a hands-on therapy that applies pressure to densified fascia, causing the fascial layers to heat up, stretch, and separate. When used in conjunction with shockwave therapy, myofascial release promotes hydration of the plantar fascia and helps to restore its slippery and elastic properties.
In a controlled randomized study, 66 patients were divided into a control group and a treatment group. The control group received sham ultrasound therapy, while the treatment group received myofascial release therapy. After 4 weeks of treatment, the myofascial release group reported a 72.4% improvement in pain and functional mobility, compared to only 7.4% in the control group.
Orthobiologic Injections
Orthobiologic solutions are concentrated natural substances, typically derived from the patient’s own cells. In severe cases of chronic plantar fasciitis, orthobiologics like platelet rich plasma (PRP) and bone marrow aspirate concentrate (BMAC) have been found to be superior to corticosteroid injections in reducing pain and restoring function.
One study compared the efficacy of PRP to corticosteroids in patients with chronic plantar fasciitis. The PRP group showed significant improvement, with results enduring for at least 24 months. By contrast, the steroid group had initial pain relief, but the results diminished over time, and were substantially lower at 24 months. Moreover, when used on already degenerating tissue, corticosteroid injections have been shown to reduce the heel’s fat pad thickness and cause plantar fascia ruptures.
Conservative care can help with pain management while the plantar fascia heals, but the recovery timeline for plantar fasciitis can be 9 months to a year or longer. According to one source, approximately 40% of plantar fasciitis patients continue to have symptoms after 2 years, regardless of treatment. For serious athletes, such a prolonged recovery period can be career-ending.
High-load strength training (HLST), is an evidence-based approach to treating chronic plantar fasciitis. The idea behind HLST is to apply a high tensile load to the plantar fascia, with the goal of stimulating collagen production to expedite recovery. By loading the Achilles tendon while simultaneously dorsiflexing the metatarsal joints, high-load tensile forces are created across the plantar fascia.
A randomized controlled trial involving 48 patients with ultrasound-confirmed plantar fasciitis divided the patients into two groups. Both groups wore orthotic shoe inserts, but one group did daily stretching while the other performed HLST every-other day for 3 months. At the 3-month marker, the HLST group reported significantly lower pain and more improved function, based on the Foot Function Index (FFI), compared to the stretching group. At 12 months, results were similar for both groups, but the HLST group experienced faster symptom relief early-on.
Following is the Standard HLST Protocol as designed by Rathleff et al:
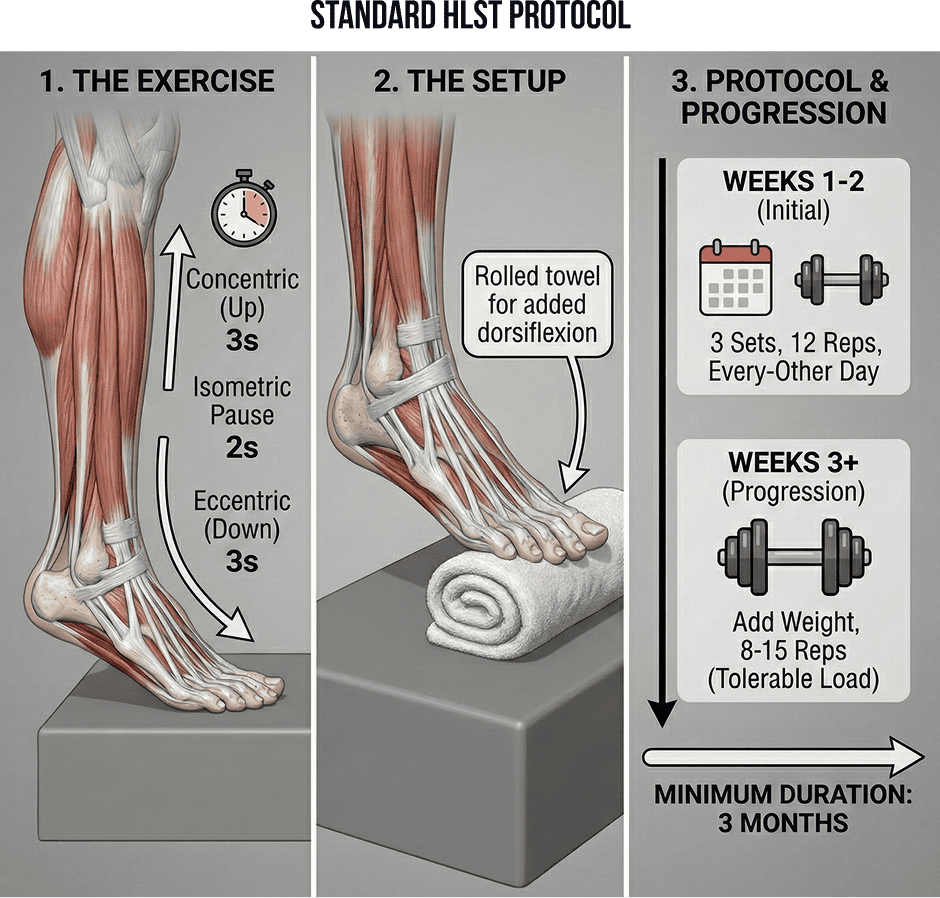
HLST has been shown to stimulate collagen synthesis, improve tissue remodeling, and enhance the plantar fascia’s ability to handle tensile stress. This protocol has also been proven effective for Achilles and patellar tendinopathies.
At NYDNRehab, we have a 100% track record of success in treating plantar fasciitis, thanks to Dr. Kalika’s expertise and 20+ years of hands-on clinical experience. We use the highest resolution ultrasonography to diagnose your condition, along with sonoelastography to assess the thickness of the plantar fascia.
Our clinic features a broad range of technologies and therapies for addressing plantar fasciitis, including orthobiologics, extracorporeal shockwave therapy (ESWT) and ultrasound guided dry needling (USDN). A recent research article published in Nature cites Dr. Kalika’s own research, highlighting USDN as a top-tier evidence-based solution for plantar fasciopathy, and ranking it alongside ESWT and PRP as a primary intervention.
In our experience, combining evidence-based treatment modalities with precision ultrasound guidance renders superior results. Our integrative and personalized approach means our patients receive the highest-quality, one-on-one customized care. Our multimodal approach to plantar fasciitis ensures quick pain relief, fast recovery, and longer-lasting outcomes.
Request an appointment»
![]()
Our location: 11 West 25th Street 5th floor, New York, NY 10010

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































