
Hip trouble may occur as a result of any one of a number of conditions and injuries associated with the pelvic area, including hip bursitis, labral hip tear, and hip flexor strain. Because the hip is centrally located and pivotal to the movement and function of the lower half of the body, injury to the hip may have serious repercussions beyond the immediate site of injury. Minors who struggle with hip pain are more likely to develop pain in the back and the joints of the lower extremities. Those who play sports, whether professionally or recreationally, are also more prone to hip injuries. Between 10 and 24 percent of injuries sustained by children while playing sports are hip-related. For all these reasons, proper diagnosis and treatment of hip pain is essential.
The largest joint in the body, the hip acquires its stability from its unique design. Because it’s a ball-and-socket joint, a special kind of joint in which the rounded surface of a bone fits neatly into the groove of another bone, it has a wider range of motion and flexibility than many other joints in the body. In the case of the hip joint, the rounded end of the thigh bone (the femur) fits into the cup-like hole of the acetabulum, the concave surface of the pelvis.
The acetabulum is a deep depression. This is important because it gives the hip joint a stability it wouldn’t have otherwise. Surrounding the head of the femur (the “femoral head”), the acetabulum helps to prevent the hip from becoming dislocated. This depression is surrounded by a rim of cartilage, the acetabular labrum, which provides a larger articular surface. This, in turn, further stabilizes the joint.
The hip region is also home to a complex, interconnected network of muscles. The quadriceps and hamstrings work in opposition to move the hip joint while stabilizing the knee. Importantly for our discussion, the three hip flexor muscles work together to flex the legs, bringing them close to the trunk. These three muscles, the iliopsoas, rectus femoris, and sartorius muscles, are vitally important in common activities like running, jumping, and cycling.
Covering the femoral head and acetabulum is a layer of articular cartilage, a rubbery substance that prevents the joints from rubbing together during movement. Also assisting in preventing friction are the bursae, tiny sacs filled with fluid resting between the tendons and bones of all the major joints. The most significant bursa in the hip is the trochanteric bursa. If it becomes inflamed, trochanteric bursitis can develop.
A proper diagnosis is critical for hip pain treatment. In most cases, bursitis occurs as a result of biomechanical abnormalities. When these abnormalities become a fixed part of a person’s gait over an extended period, they can lead to overuse injuries. For example, over-pronation (a flattening or rolling inward of the foot) can create the conditions that result in inflamed bursae. In other cases, the bursae may be injured as a result of traumatic injury.
Two of the most common types of hip bursitis are trochanteric and iliopectineal bursitis. The iliopectineal bursa, the largest bursa in the body, is associated with sports that greatly depend on the hip flexors: for example, soccer, ballet, and uphill running. Damage to this bursa can tremendously hinder the enjoyment of sports and may require groin pain treatment because of severe groin pain radiating to the thigh or anterior hip, pain so intense it may disrupt normal gait.
Trochanteric bursitis is also characterized by intense pain, though in this case the pain radiates into the lateral buttock. Patients may experience pain while standing for long periods and while climbing or running, necessitating bursitis hip treatment.
Although the labrum is designed to deepen and stabilize the acetabulum, it can also suffer damage as a result of trauma. This may happen when an athlete twists or dislocates his or her hip. Labral tears are sometimes seen in patients suffering from the effects of osteoarthritis. Symptoms of a tear may include painful clicking, a feeling that the hip is giving way beneath the patient, and pain that increases when the leg is extended. Hip labral tear treatment is generally conservative: in addition to resting, a patient may seek physical therapy and anti-inflammatory medications under the supervision of a physician.
Treatment for hip bursitis is almost always non-surgical. In the case of iliopectineal bursitis, it consists of rest, icing, and stretching of the iliopsoas. A physician may also recommend non-steroidal anti-inflammatory medication. If, however, the flexor muscle fails to respond to conservative bursitis treatment, hip injections may be necessary. The injection of corticosteroids will reduce inflammation, thereby minimizing tissue damage. In the case of trochanteric bursitis, treatment should begin with icing and heating. Phonophoresis may be used to help administer drugs through the skin to the site of injury, thus helping to control inflammation. These should be accompanied by an exercise program that includes hip abductor and core strengthening exercises. As with iliopectineal bursitis, corticosteroid injections may be necessary in more severe cases.
The iliopsoas muscle may suffer injury when a patient’s thigh is forced into extension, or blocked during flexion—as, for example, when a soccer player extending his or her leg for a kick is struck in the leg. Groin pain may develop as a result. Hip flexor pain treatment begins with rest. Gradually the patient should begin a regimen of rehabilitation within reasonable limits. If the hip flexor is torn, he or she may need to wait between four to six weeks before returning to sports.
At NYDNR we specialize in treatment of walking and running disorders. We are the first full technological gait (analysis) outpatient facility in NYC. Our C.A.R.E.N (computer assisted rehabilitation environment) is the first privately owned system in US. C.A.R.E.N’S uniqueness lies in ability to provide multisensory feedback while patient is walking, standing or balancing on one leg. C.A.R.E.N’S analytical ability allows diagnostically precise monitoring and correction of patient’s movement. We are the only clinic certified in DNS (dynamic neuromuscular stabilization) method. DNS has been remarkably successful with treatment of hip disorders, which have not responded to other physical therapy methods. For those suffering from hip bursitis and tendinosis we provide ESWT ( extracorporeal shockwave therapy)

A clinical exam and diagnostic ultrasound imaging can help your therapist pinpoint the exact location and cause of your hip and groin pain.
Ultrasound enables you and your therapist to view the hip and groin region in real time, while in motion. In addition to ultrasound, video gait analysis can help us identify faulty movement mechanics that contribute to hip and groin pain. Once the exact cause is determined, an effective treatment plan can be initiated.
Please explore more advanced diagnostic option unavailable anywhere else:

Hip dysfunction and pain can be a complex issue due to interactions of the trunk, pelvis, low back, groin and hip joint. Physical therapy and rehabilitation that is based only on subjective clinical analysis often addresses the symptoms without resolving the underlying cause.
At NYDNRehab, our groundbreaking motion analysis technology and high resolution diagnostic ultrasonography have enabled us to develop a battery of tests that perfectly reveal the dynamic functional pathology of the hip joint and pelvis. Our tests are evidence-based protocols that are considered to be the gold standard in the world of research.
Our testing protocol includes:
Combined lumbopelvic hip stability test using DLEST methodology with C.A.R.E.N., our computer assisted rehab environment
Hip joint stability test using DLEST methodology with C.A.R.E.N.
3D star excursion banner test (SEBT) for assessing the involvement of the hip joint and muscles in postural stability
3D gait or running analysis
3D kinematic joint angle analysis during a squat, lunge, drop jump and pelvis on hip rotation
Rehabilitative ultrasonography for viewing intrinsic hip stabilizing muscle activation patterns

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
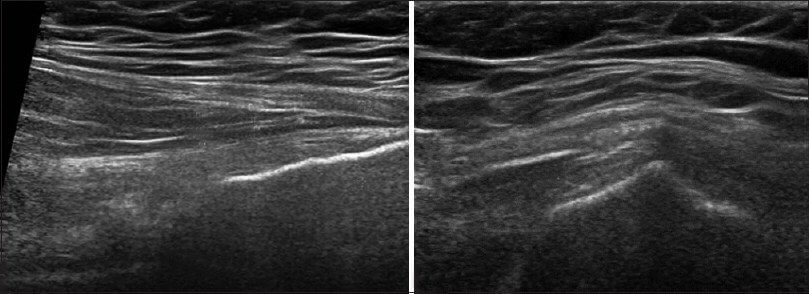
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































