December 18, 2025
The hip flexors are a group of muscles that work together to shorten the angle between your upper leg and your trunk, causing hip flexion. They act counter to the hip extensors, playing a major part in most physical activities, like walking, running, biking and swimming. Hip flexor injuries are common in sports, but they can also affect non-athletes and sedentary populations. With proper training and certain lifestyle changes, most hip flexor injuries can be avoided.
Learn about the anatomy and function of the hip flexors, common causes and types of injuries, and the most effective treatment approaches to eliminate and prevent hip flexor pain.
Hip flexion involves several key structures, including muscles, joints, and connective tissues that support and stabilize the hip.
Primary hip flexor muscles include:
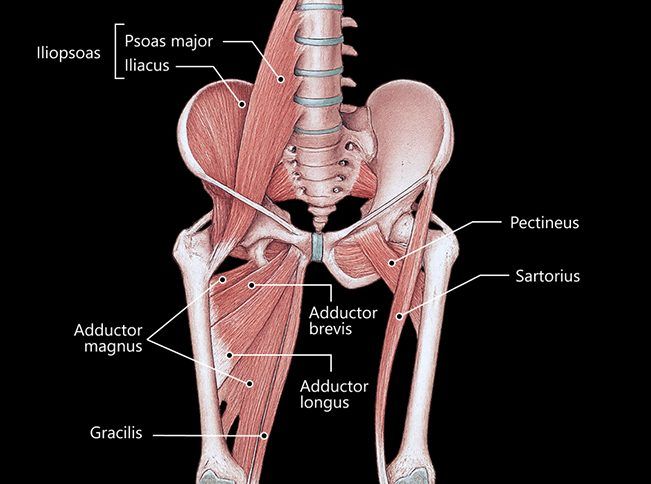
The hip joint has a ball-and-socket architecture, where the femoral head rotates within the acetabulum, allowing for hip flexion up to 140°. During flexion, the hip is supported by strong ligaments, tendons and fascia to enable force transmission and provide stability. The femoral nerve innervates the iliopsoas, rectus femoris, and sartorius, while the obturator nerve innervates the pectineus and adductor muscles. Blood to the hip flexors is supplied by the femoral and iliac arteries.
Hip flexor strains occur when the muscles or tendons in the hip flexor group – mainly the iliopsoas, rectus femoris, and sartorius – are overstretched or torn.
Common causes of hip flexor strains include:
In athletic populations, hip flexor injuries generally arise from overuse during kicking, sprinting, or rapid directional changes. Injuries to the hip flexor tendons can involve ruptures and avulsions that lead to degeneration if not properly rehabilitated.
In sedentary populations, constant sitting makes the hip flexors weak and tight, while the hip extensors become weak and lax, causing hip instability. At the same time, the core muscles also weaken, affecting the entire hip and pelvic complex, and increasing the risk of injury.
Hip flexor strains can range from mild discomfort due to overstretched muscles, to severe pain from a muscle tear or tendon avulsion. Proper assessment is key to determining appropriate treatment.
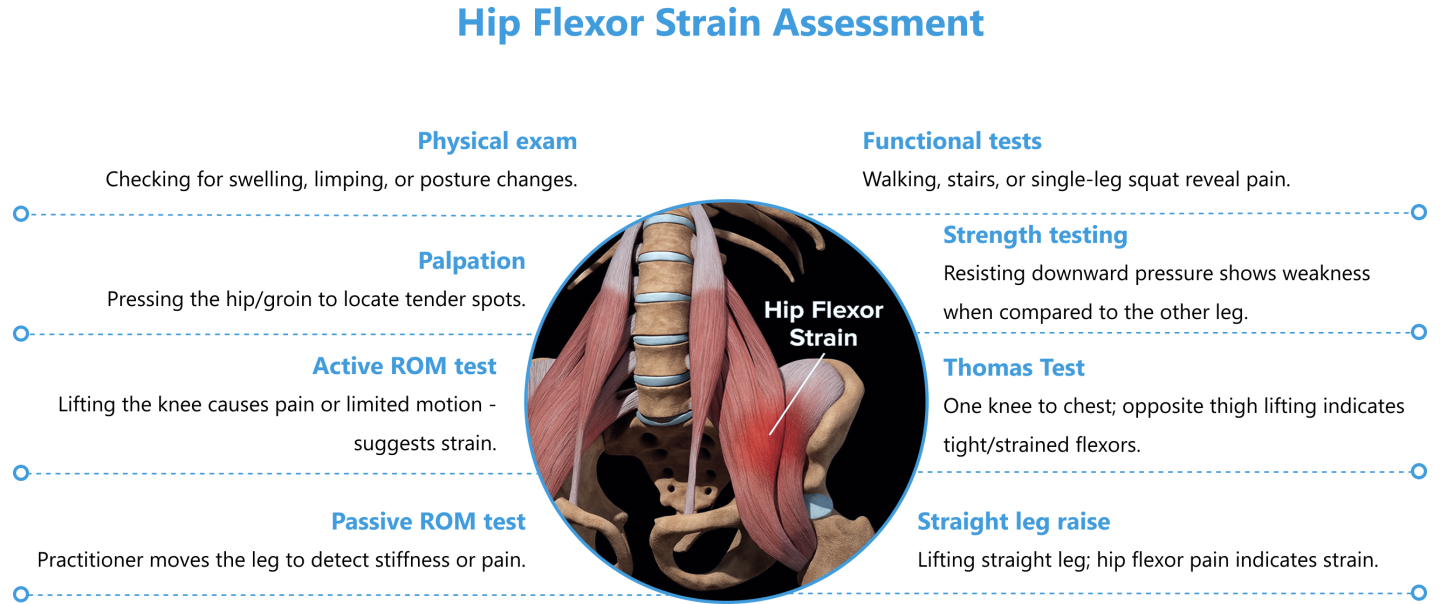
While such assessments may indicate a hip flexor strain, they cannot accurately determine the severity of the injury. Imaging with dynamic high-resolution ultrasonography allows for observation of the structures of the hip in motion, in real time. With ultrasound, we can determine if pain is generated from muscles, tendons, nerves, or a combination of causes.
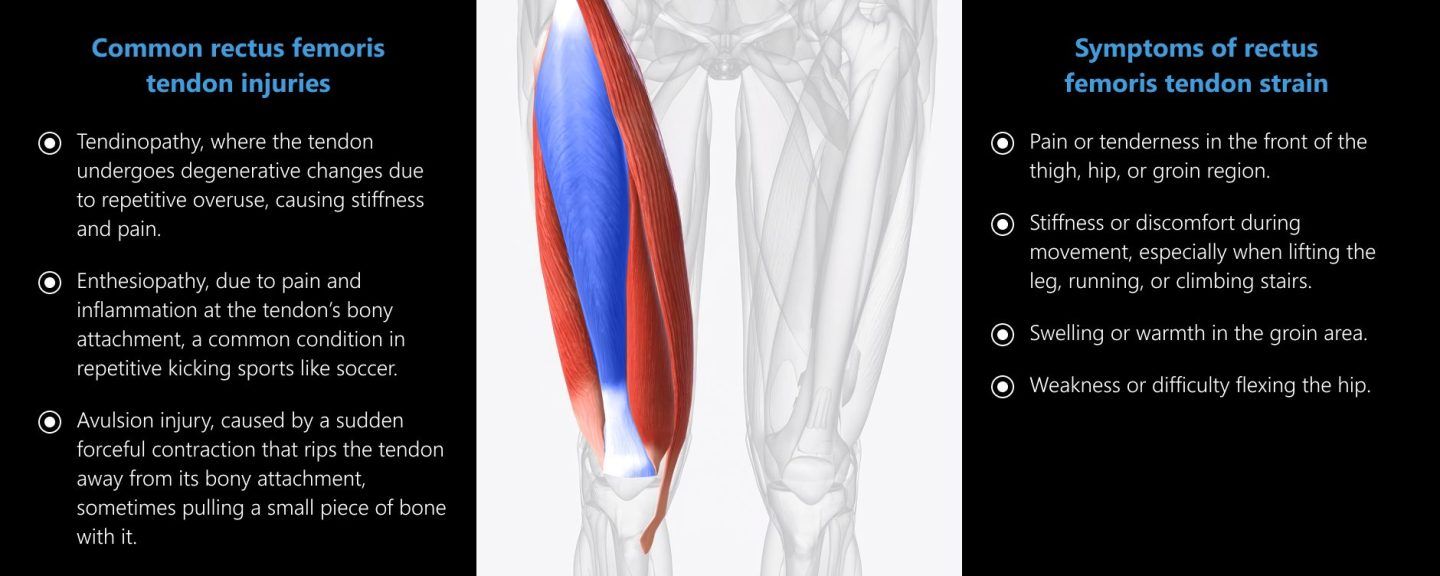
The rectus femoris muscle originates from two tendon heads – the direct head originating at the anterior inferior iliac spine (AIIS), and the indirect head originating from the superior acetabular rim. Due to its double origin and the fact that it acts at both the knee and the hip, the rectus femoris can be prone to tendon injuries that cause severe hip flexor pain.
Common rectus femoris tendon injuries include:
Symptoms of rectus femoris tendon strain include:
A tendon rupture or avulsion can cause severe pain and instability, and failure to treat tendon injuries can lead to reduced performance and ongoing tendon degeneration. When operated by a trained and experienced clinician, high-resolution ultrasonography can help to determine the exact location and severity of injury.
Treatment of hip flexor strains is aimed at reducing pain, promoting healing, and restoring function. Treatment strategies are progressive, based on the specific characteristics of the injury.
Hip flexor rehab progresses in phases:
 img class=”aligncenter size-full wp-image-152902″ src=”https://nydnrehab.com/wp-content/uploads/2016/03/Hip-Flexor-Strains-treatment-02.png” alt=”” width=”646″ height=”1080″ />
img class=”aligncenter size-full wp-image-152902″ src=”https://nydnrehab.com/wp-content/uploads/2016/03/Hip-Flexor-Strains-treatment-02.png” alt=”” width=”646″ height=”1080″ />
Recovery timelines can vary, and should not be regarded as absolute – your injury rehab should never be rushed:
Regenerative therapies and orthobiologic injections are advanced sports medicine treatments that help to accelerate tissue healing. Orthobiologic solutions are derived from the body’s own tissues or from donors, and include treatments such as platelet-rich plasma (PRP), bone marrow aspirate concentrate (BMAC), adipose-derived stem cells, and mesenchymal stem cells (MSCs).
Such therapies trigger a regenerative response at the cellular level by activating growth factors, stem cells, and signaling molecules to accelerate tissue repair, reduce inflammation, and promote soft tissue regeneration.
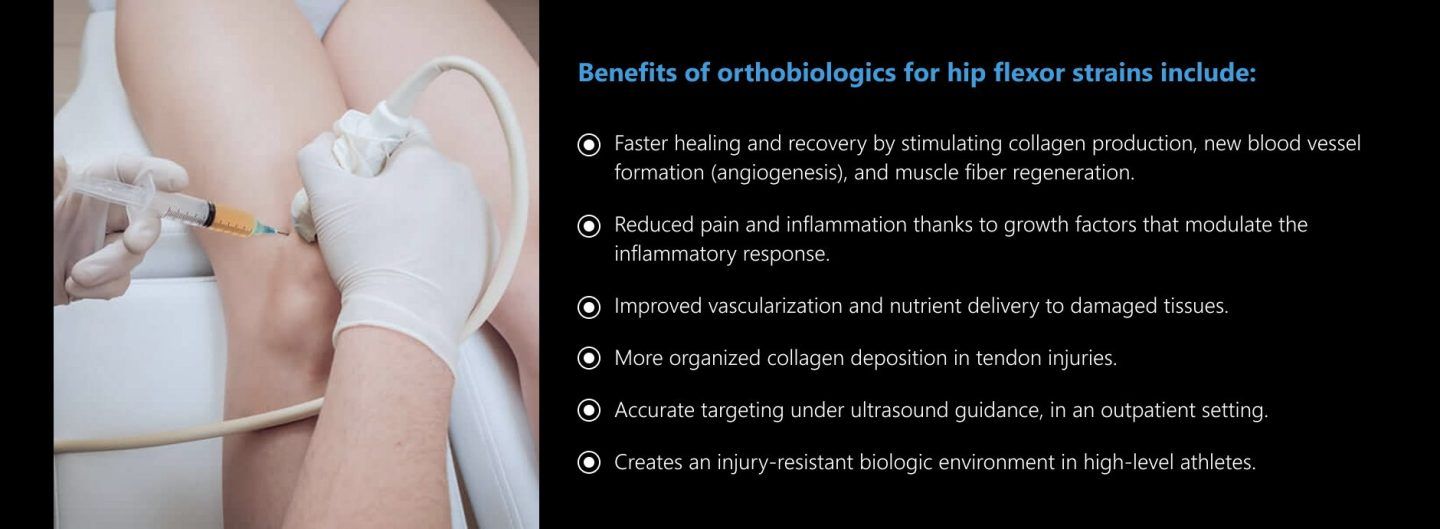
Benefits of orthobiologics for hip flexor strains include:
Extracorporeal shockwave therapy (ESWT) works synergistically with orthobiologics, adding a mechanical stimulus that activates stem cells, enhances circulation, and accelerates tissue remodeling. When combined, this dual approach can significantly accelerate healing and improve patient outcomes.
Orthobiologics are not stand-alone solutions, but they can be highly effective when used in conjunction with other therapeutic approaches. Intelligent rehabilitation takes into account the unique biomechanics of the patient and the specifics of the injury. By addressing both biological and mechanical factors, we can strive to restore pre-injury performance levels and reduce the risk of future injuries.
A successful rehab program includes:
You can dramatically reduce your risk of hip flexor injuries by adopting and adhering to a few preventative strategies:



Advancements in technology have brought with them multiple new approaches for musculoskeletal injury rehabilitation, and NYDNRehab has kept pace, offering a broad range of regenerative and orthobiologic therapies for injury healing. Our high-tech lab equips us to accurately assess your gait and biomechanics, and track your progress. Our 20+ years of experience and Dr. Kalika’s expertise in diagnostic ultrasonography make NYDNRehab the clinic of choice for hip flexor injuries in NYC.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































