Due to its unique ball-and-socket architecture, the hip and pelvic complex plays a key role in human locomotion, providing both mobility and stability, and helping to mediate load transfers between the upper and lower body. Hip pain is relatively common among adults of all ages, but it should not be accepted as a normal part of aging. Whether caused by degenerative hip disorders, trauma, or repetitive overuse, most cases of hip pain can be successfully treated with conservative holistic methodologies. If left untreated, hip pain and dysfunction can cause mechanical issues throughout the body that lead to reduced mobility and diminished quality of life.
At NYDNRehab, we use the most advanced technologies and treatment methodologies available for hip pain diagnosis and treatment. Our state-of-the-art Manhattan clinic is second to none for hip pain treatment and rehabilitation in NYC.
Clinical director & DC RMSK
Verified Expert Profiles
Dr. Lev Kalika, DC has devoted much of his life’s work to revolutionizing lower extremity pain treatment by introducing high resolution diagnostic ultrasonography for structural diagnosis, combined with gait and motion analysis technology to visualize and objectify the functional movement of the lower extremities.
Dr. Kalika has spent many years developing a unique diagnostic approach to hip pain that combines:
In addition to his clinical practice, Dr. Kalika is an accomplished researcher, with multiple peer-reviewed publications to his credit.

Orthobiologic specialist
Dr. Yuri Brosgol, MD is a neurologist with 20+ years of experience in treating adult myofascial pain. When emerging research on the critical role of fascia in human mobility captured Dr. Brosgol’s interest, he pursued training in orthobiologics and fascial release techniques. Dr. Brosgol has become a pioneer in the use of orthobiologic solutions and fascial plane hydrodissection, paving the way for transformative advancements in the treatment of myofascial disorders.
Together, Dr. Kalika and Dr. Brosgol are combining their skills to revolutionize the way myofascial pain is diagnosed and treated. By leveraging the most advanced, evidence-based approaches, they are dedicated to improving the quality of life for hip pain patients in NYC.
The hip joint is a multi planar joint surrounded by a complex network of muscles, ligaments, tendons and nerves. Conventional medical treatment for hip pain often focuses on pain management, along with physical therapy to enhance mobility and stability. But physical therapy does not provide a stand-alone solution for resolving the underlying causes of hip pain.
Hip pain can sometimes be caused by isolated conditions such as labral tears, femoroacetabular impingement (FAI), hip osteoarthritis, or bursitis, but more often it stems from the complex interplay of numerous structures in the lumbo-pelvic-hip complex, and affects multiple tissue types.
Factors that contribute to hip pain include:
Conventional treatment of hip pain often begins with physical therapy and ends with surgery, without ever addressing its root cause. We believe that successful diagnosis of hip pain can only be achieved using objective tools, and that surgery should be the absolute last resort.
We use the most advanced motion and gait analysis technology and the highest resolution musculoskeletal ultrasonography found in any private clinic in the USA to accurately identify the exact cause of your hip pain. From there, we create a customized treatment plan based on your unique diagnostic profile.
Before beginning physical therapy, we pretreat your damaged tissues, address fascial adhesions and trigger points, and restore functional joint range of motion. Only then do we begin to build strength and stability using specialized physical therapy.
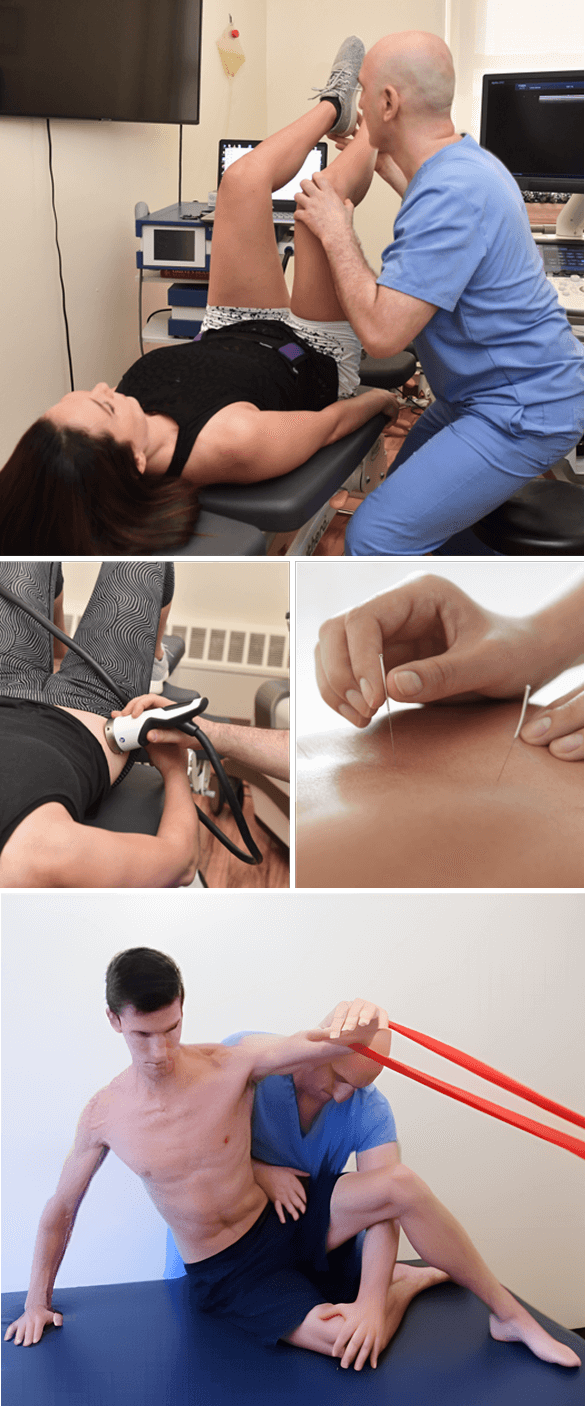
Because hip pain can stem from a number of causes and can affect multiple structures, accurate diagnosis is key to successful treatment. At NYDNRehab, we use advanced technologies to diagnose, analyze and treat hip pain and dysfunction.
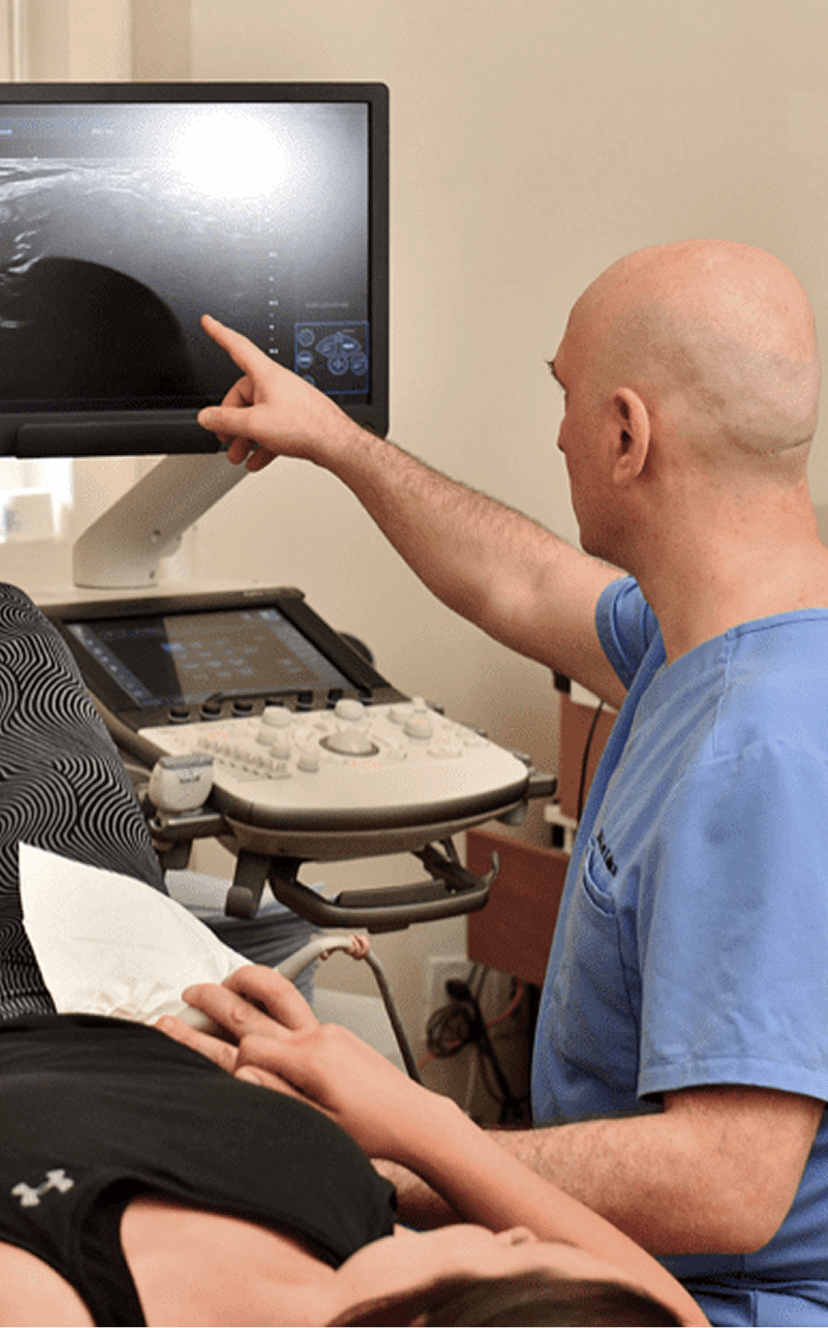
In addition to a thorough clinical exam, we use diagnostic ultrasonography to dynamically visualize tendons, ligaments, bursa, muscles, fascia and nerves that surround the hip, in real time. Your ultrasound exam takes place on your first visit, in the comfort of our clinic, with no wait time for lab results.
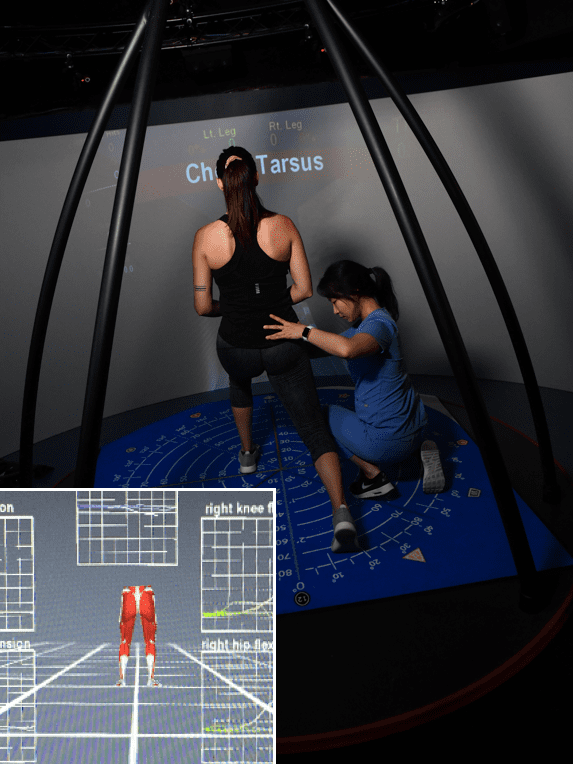
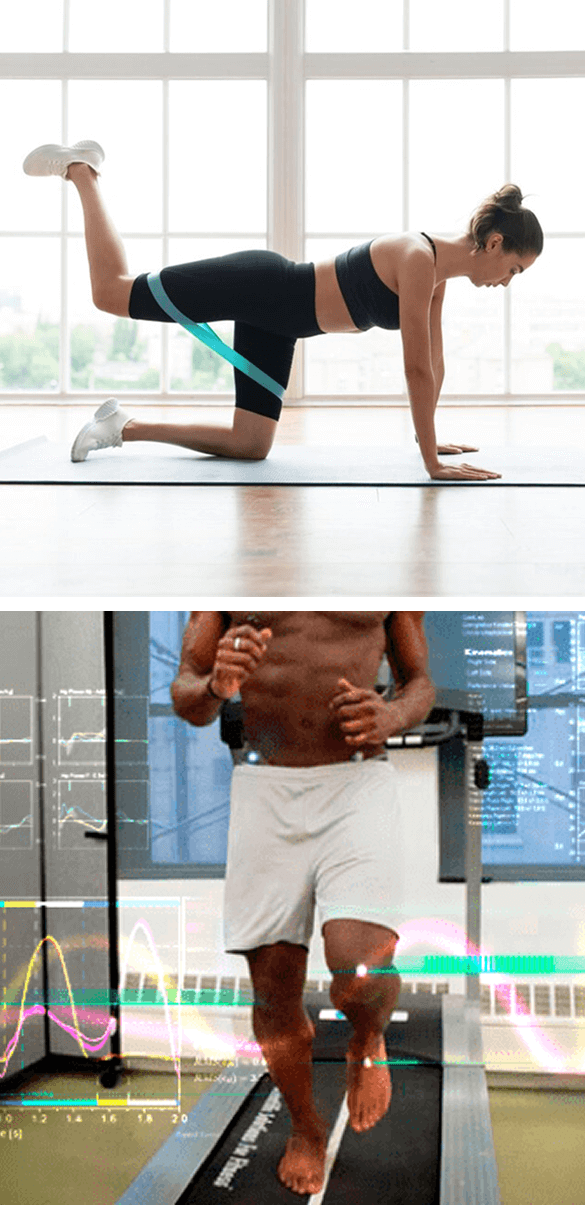
Our sophisticated video gait analysis technology empowers us to visualize and measure ground reaction forces, joint kinematics, muscle firing patterns and other quantitative parameters, to get a clear functional overview of the hip, pelvis and lower kinetic chain.

In addition to ultrasound imaging and gait analysis, our assessment protocol includes:
We use your collected data to create a baseline and a personalized treatment plan, We monitor your progress every step of the way, to ensure you get the fastest and most effective results.
Hip tendonitis
Femoroacetabular impingement (FAI)
Hip labrum tears
Adult hip dysplasia
Running hip pain
Hip flexor strains
Snapping hip syndrome
SI joint pain and dysfunction
Post-surgical hip replacement pain and rehab
Hip fracture rehabilitation
Femoral head stress fractures
Fascia is a complex network of connective tissues that surrounds and connects structures, tissues and organs throughout your body. Fascia works together with muscles to guide and control movement, and mediate outside forces. Together, muscles and fascia – aka the myofascial system – creates tensegrity that plays a key role in hip mobility and stability.
Fascia is rich with nerve endings, and capable of transmitting stronger tension and pain signals than muscle tissue. Healthy fascia is made up of collagen and hyaluronic acid, making it tough, elastic and slippery. But fascia is highly adaptive to chronic tension or injury, which can lead to fascial thickening, making it dense, sticky and inelastic. When damaged, it can adhere to other structures, entrapping nerves and blood vessels and preventing them from gliding.
Fascial densification can interfere with muscle action, restricting mobility and causing pain. Densified fascia can pull on adjacent structures, creating a feedback loop of widespread pain and tension in other areas of the body that doesn’t align with the locus of hip pain.
In cases of musculoskeletal pain, treatment strategies that do not consider and address the role of fascia are destined to fail, because fascia plays an integral role in all aspects of human mobility.

Identifying and treating underlying issues prior to beginning physical therapy is key to getting fast and effective results. Failure to pre-treat your condition can completely undermine your treatment protocol, and in some cases, your condition may even worsen.
At NYDNRehab, we use a broad range of regenerative technologies and integrative therapeutic approaches to resolve issues that can stand in the way of successful physical therapy.
Our staff is certified in a diverse array of holistic treatment methodologies, and our one-on-one treatment sessions are personalized, based on your unique diagnostic profile. Once we pre-treat your damaged tissues and eliminate compensation patterns, your hip will be ready for physical therapy.
The human body has its own innate healing mechanisms, but it sometimes needs a nudge to accelerate the healing process. Regenerative technologies help to jump-start healing by stimulating tissue repair at the cellular level. Our outpatient regenerative therapies expedite recovery with minimal discomfort for the patient.
Focused ESWT is used as a regenerative treatment for damaged tendon, muscle and bone tissue. This technology produces high frequency sound waves to stimulate the body’s own reparative mechanisms. It is especially effective for chronic degenerative tendon disorders and myofascial pain syndrome.
EMTT is a fairly new technology that transmits high energy magnetic pulses to targeted tissues. The magnetic waves synchronize with the body’s own magnetic fields, causing a disturbance that triggers a regenerative response. EMTT waves can penetrate deep tissues up to 18 cm beneath the skin’s surface, to target difficult-to-reach tendons, muscles, bones and nerves.

EPAT, also known as defocused shock wave therapy, uses acoustic pressure waves to enhance blood circulation to targeted tissues. This speeds up the delivery of oxygen and nutrients to damaged tissues and stimulates cellular metabolism, to accelerate the healing process.
HEIT uses electromagnetic fields to penetrate cells, tissues, organs and bones, to reactivate the electrochemical function of cells and cell membranes. HEIT generates a magnetic field 600 times stronger than the field of a normal magnet, to stimulate healing of nerves, muscles and blood vessels.

Our INDIBA Tecar therapy machine converts electrical current into a stable radio frequency current of 448 kHz, designed to increase and stabilize the exchange of ions in damaged cells, evoking a regenerative response that accelerates healing. INDIBA can be used to successfully treat joint and muscle disorders, low-back pain, sports injuries, surgical incisions and various pain syndromes. Another therapeutic effect of INDIBA is extreme and prolonged cellular hyperthermia. Due to this effect, INDIBA therapy combined with manual therapy and soft tissue tissue manipulation enables instantaneous release to occur, significantly shortening the number and duration of physical therapy sessions. What is normally accomplished in two months of physical therapy can be accomplished in 3-4 sessions with INDIBA.
Myofascial trigger points often contribute to lower back pain. Dry needling is an outpatient procedure that inserts non-medicated needles into the trigger point to evoke a twitch response, releasing the trigger point and immediately relieving pain. Ultrasound guidance eliminates the need for multiple insertions, reducing pain and discomfort for the patient.

Injection therapies use natural/neutral solutions that stimulate cellular repair by either nourishing or irritating the targeted cells. Guidance by ultrasound ensures that the injected substances hit their mark, for maximum effectiveness.

PRP therapy uses a sample of the patient’s own whole blood, which is spun in a centrifuge to extract a high concentration of platelets. When injected into damaged tissues, PRP initiates tissue repair by releasing biologically active factors such as growth factors, cytokines, lysosomes and adhesion proteins. The injected solution stimulates the synthesis of new connective tissues and blood vessels. PRP can help to jump-start healing in chronic injuries and accelerate repair in acute injuries.
Prolotherapy uses a biologically neutral solution, often containing dextrose, saline or lidocaine. The solution irritates the affected connective tissue, stimulating the body’s own natural healing mechanisms to encourage growth of new normal ligament or tendon fibers.

A strong and stable hip and pelvic region is fundamental to long-term mobility. Once hip pain becomes chronic, it can set off a cascade of issues that affect structures throughout your body. In response to chronic pain, you are likely to develop compensation strategies to offload the affected hip.
As pain persists, compensation patterns can become habitual, affecting your spinal and joint alignment anywhere along the kinetic chain. This can result in inefficient muscle recruitment patterns, fascial densifications, and nerve compression that sends pain signals to the brain.
To avoid chronic hip pain, adopt these positive strategies:

Hip pain can be debilitating, interfering with your ability to enjoy life to its fullest. Pain medications and surgeries often fail to get to the root cause of hip pain, addressing the symptoms without resolving their underlying causes. At NYDNRehab, our goal is to get to the source of your hip pain and correct it, so you can move freely, without pain or dysfunction. Our advanced approaches, expertise and personalized treatment programs make NYDNRehab the premier clinic for hip pain treatment in NYC.





These case studies reflect real clinical conditions evaluated at NYDNRehab using advanced diagnostic methods and individualized rehabilitation strategies. All cases are evaluated and managed by Dr. Lev Kalika and the NYDNRehab clinical team.























 Dr. Yuri Brosgol
MD
Dr. Yuri Brosgol
MD
 Dr. Michael Goynatsky
DPT
Dr. Michael Goynatsky
DPT
 Dr. Daniela Escudero
DPT
Dr. Daniela Escudero
DPT
 Dr. Michelle Agyakwah
DC
Dr. Michelle Agyakwah
DC
 Dr. Tatyana Kapustina
L. Ac.
Dr. Tatyana Kapustina
L. Ac.

Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination





















