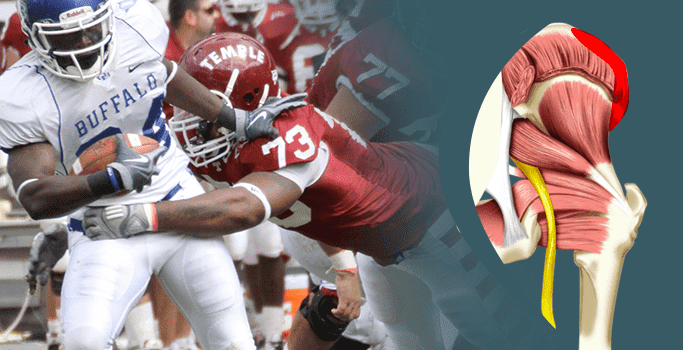
A hip pointer wound is a very common injury received by athletes or people playing sporting activities. Defined as a contusion or bruise on the upper portion of the hip bone, known by the medical term iliac crest, a hip pointer is often accompanied by a second wound on the abdominal muscles. Many people mistakenly believe that it is the hip bone that becomes wounded but it is actually the connecting muscle tissue that gets injured in a hip pointer injury.
Hip pointer injuries can usually be detected right away, expressed by severe discomfort in the groin, side of the body around the area of the hip, and associated exterior bruising. The discomfort felt in the hips can be quite strong, exacerbated when the injured person walks, laughs, sings, coughs, or even breathes deeply. The hip pointer wound causes a minor amount of internal bleeding in the muscle tissues that surround the hip. These muscles then become inflamed and start to expand, causing any movement of the associated leg to be quite uncomfortable.
Hip pointer wounds are most commonly sustained by people who play contact sports, including American football, skiing, lacrosse, cycling, and hockey. A direct strike against the top, outer part of the hip can lead to a bit of the bone being clipped off. These types of wounds can result as either a hard strike from another person, a ball, or by falling to the ground and ramming against a hard surface.
While few hip pointer wounds become serious enough to merit specialized medical care, these types of wounds require a significant amount of rest to create the conditions for proper healing. Sports medicine experts estimate that it takes between one and seven weeks for an individual with a hip pointer wound to fully recover from the injury to their hip bone, hip muscles tissues and ab muscles.
Any person who engages in aggressive or high-velocity sports and fails to wear protective cushioning on their hips is at the highest risk of sustaining a hip pointer wound. Athletes who play American football are statistically most likely to sustain a hip pointer wound due to the nature of the sport which involves hard blows to the hip from other players, especially from their helmet or hardened shoulder pads. American football players are also at a higher risk of developing this type of wound because tackles can involve a hard slam against the ground.
Other types of vigorous play, including lacrosse, soccer, gymnastics, hockey, skiing, and bicycling can also precipitate an increased risk of developing a hip pointer wound due to the frequent nature of either hard blows received from other players and/or balls or slamming against the ground and landing on an unyielding surface.
Hip pointer wounds are rarely diagnosed in a doctor’s office. A number of symptoms can indicate the presence of a hip pointer injury, including:
Most hip pointer wounds can be treated without emergency medical intervention. The standard recommended treatment for a hip pointer wound is to rest for the first 48 hours. During the first two or so days, it is recommended that anyone who sustained a hip pointer wound apply cold packs for 20-25 minutes on a schedule of three to four times a day as long as the cold is not applied directly to naked skin. It is also counseled to maintain the injured hip and/or leg elevated for the first day or so.
Starting on the third day, the standard course of treatment for a hip pointer wound is to begin to slowly and gently stretch the area, focusing on strength-building routines to add flexibility and power back to the area. Some individuals with a hip pointer wound find it advantageous to take over the counter pain drugs like ibuprofen to minimize discomfort and tenderness.
While there is usually no long-term damage associated with hip pointer wounds, receiving a blow or taking a tumble can result in a very uncomfortable condition. Anyone who received a hip pointer injury will have to carefully begin to apply physical therapy techniques to recover their full range of flexibility. Some physical therapists recommend using special massages and movement exercises once the primary discomfort of a hip pointer wound has faded away. In some severe cases, it may be necessary to receive a corticosteroid solution inserted into the area in order to minimize tenderness and inflammation and hasten full use of that region of the body.
Surgical intervention for a hip pointer injury is extremely rare and should only be undertaken if there is a confirmed diagnosis that a significant bone fracture has been sustained.
Sports medicine authorities recommend that injured athletes begin a course of physical therapy as soon as possible in order to minimize down time. They recommend a number of stretching and movement routines, including:

A clinical exam and diagnostic ultrasound imaging can help your therapist pinpoint the exact location and cause of your hip and groin pain.
Ultrasound enables you and your therapist to view the hip and groin region in real time, while in motion. In addition to ultrasound, video gait analysis can help us identify faulty movement mechanics that contribute to hip and groin pain. Once the exact cause is determined, an effective treatment plan can be initiated.
Explore more advanced diagnostic tools available only at NYDNRehab:

Hip dysfunction and pain can be a complex issue due to interactions of the trunk, pelvis, low back, groin and hip joint. Physical therapy and rehabilitation that is based only on subjective clinical analysis often addresses the symptoms without resolving the underlying cause.
At NYDNRehab, our groundbreaking motion analysis technology and high resolution diagnostic ultrasonography have enabled us to develop a battery of tests that perfectly reveal the dynamic functional pathology of the hip joint and pelvis. Our tests are evidence-based protocols that are considered to be the gold standard in the world of research.
Our testing protocol includes:
Combined lumbopelvic hip stability test using DLEST methodology with C.A.R.E.N., our computer assisted rehab environment
Hip joint stability test using DLEST methodology with C.A.R.E.N.
3D star excursion banner test (SEBT) for assessing the involvement of the hip joint and muscles in postural stability
3D gait or running analysis
3D kinematic joint angle analysis during a squat, lunge, drop jump and pelvis on hip rotation
Rehabilitative ultrasonography for viewing intrinsic hip stabilizing muscle activation patterns

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
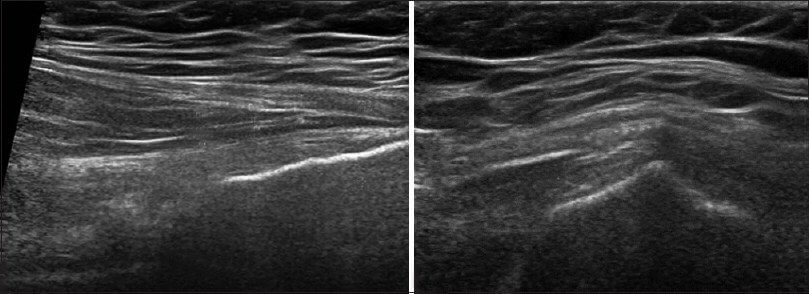
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































