October 27, 2025

Joint and back surgeries are on the rise, not only in the United States but around the world. Yet surgical interventions are costly and pose substantial health risks, with no guarantee of successful outcomes. In many cases, surgical outcomes are no better, and sometimes worse than, the outcomes of conservative care. Meanwhile, the cost of medical services has gone through the roof in an era when the health of Americans is at an all-time low.
Gain insight into the issues plaguing mainstream medicine, the dramatic uptick in unnecessary procedures, and breakthrough holistic alternatives that deliver superior results.
It is impossible to explain the increase in unnecessary procedures without addressing the twin elephants in the room: The rising cost and diminishing quality of healthcare in the United States.
We can point to three primary factors driving these phenomena:
Prior to the 1970s, the core mission of healthcare in the US was providing quality patient services. Doctors had a great deal of autonomy in decision-making, and patients were free to select their healthcare providers and services based on individual needs and preferences. Healthcare costs were reasonable, and medical-driven bankruptcies were rare.

Enter the HMO Act of 1973, whose stated intent was to to improve patient care, decrease health care costs, and emphasize preventative health care, all through the implementation of Health Management Organizations, or HMOs.
Fast-forward 50 years, and we see sky-high costs for insurance premiums and inflated prices for medical services at every level, with soaring out-of-pocket costs for patients, even among the fully insured.
Healthcare entities attribute the rising cost of patient services to multiple factors:
What they don’t disclose is that the number of hospital administrators has mushroomed in the 21st Century, accounting for a substantial portion of rising healthcare costs.
According to an article in the Harvard Business Review, the number of US healthcare workers increased by 75 percent between 1990 and 2012, but up to 95 percent of new jobs were administrative positions not directly involved in patient care.
Clearly, any organization top-heavy with administrators is going to reflect the cost in its bottom line, and the onus of offsetting costs trickles down to consumers, both patients and taxpayers. Meanwhile, HMOs, not doctors, determine which interventions are deemed necessary, and which are eligible for benefit payouts.
Consider the following facts:

Despite the high cost of US healthcare, Americans today are more unhealthy than ever, and the quality of patient care has declined dramatically over the past 50 years.
One can safely assume that many consumers adopt a “bang-for-the-buck” mentality, seeking more healthcare services, including expensive and unnecessary surgeries, to justify the hefty cost of health insurance premiums.
According to US government statistics, an estimated 7.5 million unnecessary medical and surgical procedures are performed each year in the United States, with about 8.9 million unnecessary hospital stays.
Hospitals and doctors are often incentivized and even bullied by administrators into maximizing revenues per patient, leading to unnecessary procedures and treatments, accompanied by diminished personalized care.
The typical patient journey goes something like this:
One important job of hospital administrators is to negotiate with HMOs for the best rate of return on patient services. This ensures that both the hospital and the HMO optimize profits. Unfortunately, such negotiations often leave quality of patient care out of the loop, forcing doctors to compromise in their treatment protocols.
During COVID, hospitals lost significant revenues when elective surgeries were put on hold. To offset losses, many hospitals looked to the older adult population, performing record numbers of surgeries that were of little benefit to patients.
In addition to HMO payouts, hospitals stand to profit from Medicare and Medicaid, government programs designed to support aging Americans and the underprivileged. These programs are easy to exploit and are often the target of fraud. Unnecessary surgeries charged to such programs are a cash cow for unscrupulous practitioners.
According to a report by CNBC, taxpayers dished out over $100 billion in Medicaid and Medicare fraud in 2022, and a report from the LOWN institute revealed that over 100,000 older Americans got unnecessary surgeries during 2020, the first year of COVID.
For more than a century, the fields of integrative and holistic medicine have faced pushback from what we now accept as mainstream medicine. Prior to 1910, homeopathy, herbal medicine, chiropractic, and naturopathy were commonplace in America.
The shift away from natural solutions and toward allopathic medicine began in 1910 with a document called the Flexner Report, commissioned by the Council on Medical Education, a body created by the American Medical Association. The Flexner report was funded by the Rockefeller Foundation and the Carnegie Foundation for the Advancement of Teaching.
In essence, the Flexner Report drew the following conclusions:
After the Flexner Report’s publication, the US Congress implemented changes to make allopathic medicine the universal standard of care in America, and Rockefeller and Carnegie proceeded to fund medical schools across the country under the condition that they only teach allopathic medicine.
Today, after decades of underwhelming outcomes and the failure of “wonder drugs” to live up to their hype, the health of Americans has rapidly declined while the healthcare industry has flourished and become bloated.
Now, a growing number of patients are taking responsibility for their own health, wresting it away from allopathic doctors and seeking more holistic solutions that do not involve drugs or surgery. Consequently, the alternative medical community is seeing a resurgence, backed by new technolog
Many joint and back surgeries have little to no scientific evidence to support them, yet they are performed by the thousands each year. Some routine surgeries have been performed for decades with no better outcomes than physical therapy and regenerative treatment.
In many cases, the side effects of surgery are worse than the original condition. Sadly, surgeons tend to downplay negative side effects and often fail to disclose realistic recovery timelines.
Following are some of the most commonly performed surgical procedures that are often unnecessary and frequently do patients more harm than good:
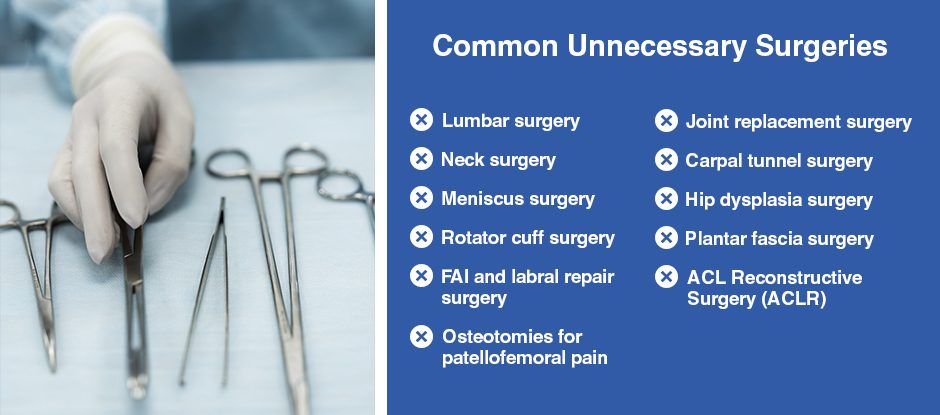
Other than traumatic injuries, joint and back pain is almost always caused by factors that can be corrected without surgery. Pain often arises from compression or entrapment of nerves by other structures, and can be alleviated by correcting posture, rebalancing muscle tension, eliminating myofascial trigger points, and reducing local and systemic inflammation.
Lifestyle factors are frequently to blame for back and joint pain, such as:
Metabolic disorders and systemic inflammation are often symptomatic of poor lifestyle choices, and can lead to osteoarthritis and neuropathies that affect joints and vertebrae. Lifestyle factors can also lead to fascia densification and nerve compression/entrapment that contribute to joint and back pain.
Certain types of medications can also cause joint pain. According to Aetna Medicare Solutions, commonly prescribed medications that cause joint and muscle pain include:
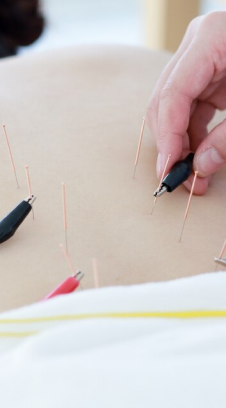
Physical therapy, fascia manipulation therapy, ultrasound-guided dry needling and shockwave therapy are all evidence-based alternatives to surgery that are highly effective and pose minimal risks to patients. Patient satisfaction tends to be higher with conservative care, and outcomes are often as good as or better than surgery.
When coupled with lifestyle modification, alternative therapy can stop the downward spiral of physical decline and set you on a path to improved health and enhanced mobility.
Joint and back surgery carry with them high risks, with no guarantee of success. When you factor in the many drugs involved, the declining standards of patient care, and the out-of-pocket expenses incurred by the patient, most surgeries should be an absolute last resort.
Thankfully, new technologies and a plethora of new research are paving the way for alternative therapies and treatment approaches that put patients above profits.
Following are just a few:
Cross-Bracing Protocol (CBP) for ACL Ruptures
A common long standing belief in medical circles is that the knee anterior cruciate ligament (ACL) is so bereft of blood flow that it has a limited capacity for self-healing. But new research published in 2023 is dispelling that belief with a new approach to treating ACL ruptures called the Cross-Bracing Protocol (CBP).
Contrary to past consensus, the researchers argued that the ACL actually has a rich vascular supply, and while it is slow to heal, the main barrier to natural healing is the gap between ligament fragments after a rupture. They observed that the distance between the ACL origin to its insertion is shortest at knee flexion of 90°–135°, and theorized that by shortening the ACL to 90º, the gap between ligament fragments would be eliminated, and the ACL would be able to self-heal.
To test their hypothesis, the research team studied 80 patients within 4 weeks of their ACL rupture, fitting them with a knee brace that immobilized the injured knee at 90° for 4 weeks, thereafter gradually increasing the joint angle at weekly increments until the brace was removed at 12 weeks. During and after CBP, patients were treated with physical therapy rehabilitation. At 3 months post-rehab, 90% of patients showed evidence of ACL healing on MRI.
This study is just one example of strides being made by researchers to find alternative natural solutions to joint injuries that don’t involve drugs or surgery.
Other recent innovations in rehabilitative medicine include:
In addition, a wealth of regenerative technology is emerging that dramatically reduces pain and inflammation and accelerates healing by tapping into the earth’s electromagnetic fields, sound waves, radio frequencies, and the body’s innate healing mechanisms.
Examples include:
With many more holistic approaches on the horizon and a growing interest in alternative therapies, greater numbers of patients are likely to venture away from allopathic medicine and seek integrative healthcare for back and joint pain.
Many physical therapy clinics and chiropractors advertise alternative medical services, but only a handful have the training, experience, and expertise to effectively treat a broad range of musculoskeletal disorders. In addition, few private clinics feature research-grade technologies for imaging, diagnosis, analysis and advanced therapeutic treatment.
At NYDNReb, we pride ourselves on providing holistic and personalized patient services that are second to none. We believe that pain-free movement is essential to quality of life, and that what cannot be measured cannot be successfully treated.
Our cutting-edge technologies combined with world-class expertise make NYDNRehab the clinic of choice for alternative holistic patient care, without drugs or surgery.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination