
Soft tissue injuries are often treated with a one-size-fits-all approach that does not take into account the unique anatomy, muscle architecture and cellular responses of the individual patient. In many cases, in the early post-injury phase, attention is focused on symptom management while ignoring healing processes on the molecular and cellular levels.
In the rehabilitative phase, physical therapy exercises are often prescribed based on research, most of which is conducted on young healthy college students. Little attention is paid to how individual muscles and muscle chains react to rehab exercises in terms of of muscle recruitment and firing patterns. Injuries can alter muscle architecture in ways that impact movement mechanics and function.
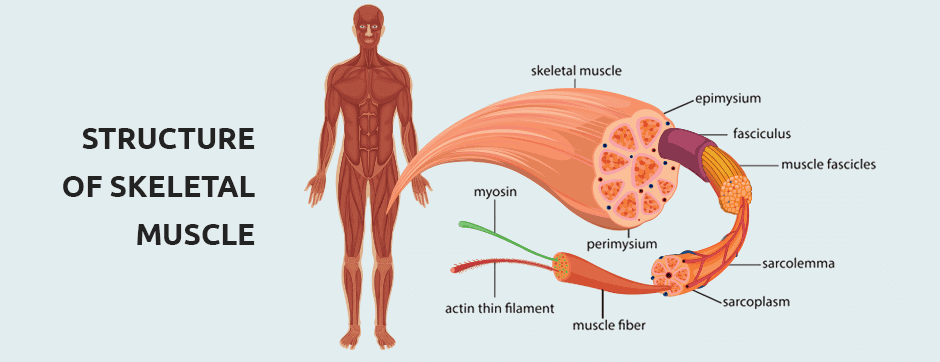
On a microscopic level, muscle fibers are single cells with the capacity to shorten in response to a neural stimulus via a series of chemical reactions. Muscle fibers are bound into contractile units called fascicles by a fibroelastic perimysium. Muscles are attached to bones by tendons and aponeuroses, and the entire muscle complex is held in place by a thin tough sheath of fascia. The architecture of skeletal muscle is defined by the way muscle fascicles are arranged relative to the muscle’s axis of force production, and the angle at which they attach to the tendon. The architecture of individual muscles varies, depending on the muscle’s location and function.
Some fascicles, like those of the biceps brachi, run the length of the muscle, parallel to the longitudinal axis. They have a relatively large range of motion but do not generate a lot of force. Penniform fascicles like those of the deltoid, rotator cuff and calf muscles, approach the tendon at oblique angles. As tension is generated in the muscle fibers, the angle of pennation increases. The unique arrangement of penniform muscles limits their range of motion, but they can generate a lot of force for their size.

Muscle injuries, immobilization and subsequent surgical repairs can temporarily or permanently alter muscle architecture, depending on the degree and nature of damage. Targeted eccentric exercise training and other training modalities like the Kineo intelligent loading system can help to restore altered muscle architecture.
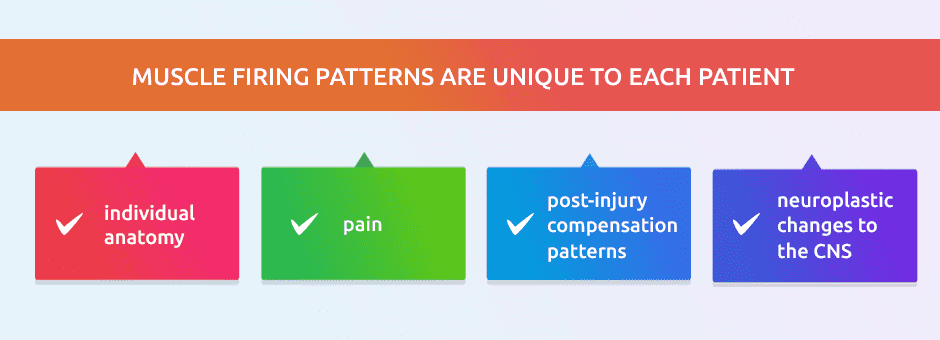
Muscle injury also affects neuromuscular pathways due to protective neuroplastic changes in the central nervous system. Those changes can alter muscle recruitment and firing patterns, and need to be addressed as part of the rehabilitative process. Achieving optimal recruitment patterns is critical to full restoration of muscle function after an injury.
Conventional treatment of soft tissue injuries centers on managing symptoms in the early stages and progressive loading exercises in the rehabilitation stage, to restore muscle strength and joint range of motion. Although strength and range of motion are important, they fall short of restoring optimal function, because they do not address architectural and neuroplastic changes. In order to fully assess tissue damage and monitor recovery, we must be able to look at the damaged tissues themselves. High-resolution ultrasonography performed in real time enables us to visualize muscles, tendons, and neural bodies with the patient in motion. In addition, we are able to assess muscle recruitment and firing patterns using surface techniques.
Muscle firing patterns are unique to each patient, and vary by:
NYDNRehab has acquired the most sophisticated Apollo ultrasound machine available, to visualize muscle architecture and pennation angles in real time. The Apollo gives us the added benefit of sonoelastography to assess and monitor the healing process.
Our dedication to personalized patient care, along with ultrasonography, virtual reality feedback and other advanced technologies, sets our clinic apart as the best injury rehab clinic in NYC.
Resources
Hayashi, Ikuta, et al. “Change in the pennation angle of the supraspinatus muscle after rotator cuff tear repair.” Journal of shoulder and elbow surgery 28.5 (2019): 888-892
Timmins, Ryan G., et al. “Architectural adaptations of muscle to training and injury: a narrative review outlining the contributions by fascicle length, pennation angle and muscle thickness.” British journal of sports medicine 50.23 (2016): 1467-1472.
Ward, Samuel R., et al. “Plasticity of muscle architecture after supraspinatus tears.” Journal of orthopaedic & sports physical therapy 40.11 (2010): 729-735.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































