
Stability and mobility are mechanical properties that define the quality of human movement. When finely tuned, mobility and stability complement one another, allowing for optimal joint range of motion without risk of injury. But when mobility dominates stability, movement is impaired, subjecting the body to pain and dysfunction that leads to disability.
In average people, excessive joint mobility may be acquired from activities like gymnastics, ballet or yoga that deliberately stretch stabilizing structures — muscles, tendons and ligaments — beyond their functional range of motion. Those people often experience pain and dysfunction later in life that can be mitigated with physical therapy. However, certain conditions are inherited, as is the case with Ehlers-Danlos syndrome, a hypermobile disorder that affects roughly 3% of the population.
This Guide provides basic information about hypermobile Ehlers-Danlos syndrome (hEDS), to help patients better understand the condition and what can be done to treat it.
Ehlers-Danlos syndrome (EDS) is an umbrella term for 13 rare subtypes of inherited connective tissues disorders. Of the 13 subtypes, hypermobile EDS is the most common, accounting for up to 90% of all EDS cases.
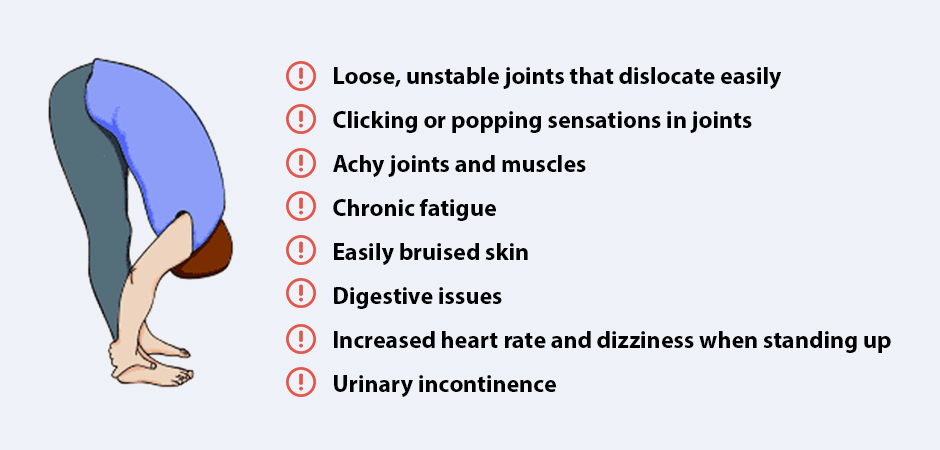
hEDS is characterized by:
Loose, unstable joints that dislocate easily
Clicking or popping sensations in joints
Achy joints and muscles
Chronic fatigue
Easily bruised skin
Digestive issues
Increased heart rate and dizziness when standing up
Urinary incontinence
Many of the subtypes of EDS are associated with specific gene mutations that affect collagen synthesis. However, researchers have not been able to identify a genetic basis for hypermobile EDS.
While the condition is rare, it can pose real problems for both children and adults with hEDS. Movement can be clumsy and awkward, challenging balance and increasing the risk of falls and injury. Participation in sports and exercise is limited, and hEDS sufferers may be subjected to social ostracism.
Early diagnosis and treatment can improve joint stability and equip patients with strategies for enhancing movement quality and reducing injury risk.
In patients with hypermobile EDS, muscles and connective tissues that support and stabilize the joints are abnormally distensible and hyper-responsive to force loads. People with hypermobile EDS are often called “double-jointed” because their joints are able to move beyond normal functional range of motion.
Because symptoms of hEDS often overlap with other pain syndromes and disorders, such as fibromyalgia, the condition can be difficult to diagnose, especially for clinicians who have never encountered hEDS.
In 2017, the International EDS Consortium revised their diagnostic criteria for all 13 subtypes of EDS, including hypermobile EDS.
According to 2017 EDS international guidelines, diagnosis of hypermobile EDS requires the simultaneous presence of three sets of criteria:
1. Generalized joint hypermobility
2. Family history of hEDS
3. Absence of other neuromuscular disorders
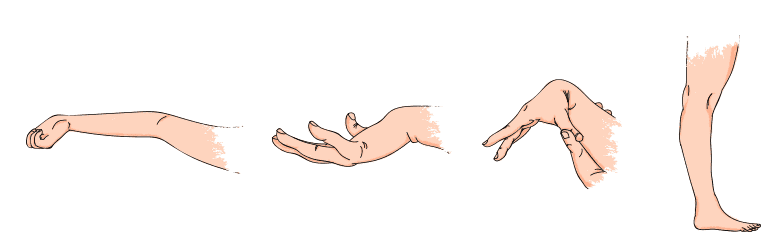
To determine the degree of joint hypermobility, clinicians use the Beighton Score, a nine-point scoring system that measures joint flexibility of the thumbs, pinky fingers, knuckles, elbows, knees and spine. The higher the score, the greater the degree of hypermobility. An hEDS diagnosis requires a Beighton Score of 6 or greater for children, 5 or greater for adults under 50, and 4 or greater for adults over 50.
In addition to those criteria, certain coexisting symptoms may signal the presence of hEDS, including:
Chronic fatigue
Sleep disorders
Gasto-intestinal distress
Autonomic nervous system dysfunction
Anxiety and depression
Your doctor may also use the Dynamic Integrative Model for Fascia to evaluate your condition, along with the Spider Symptom Severity Scale to evaluate the impact of hEDS on various body systems.
Recent studies reveal that hEDS patients have reduced proprioception — the patient’s awareness of their body’s position relative to gravity. Proprioception is mediated by mechanoreceptors (proprioceptors) located in muscles, joints, connective tissues and fascia.
Because proprioceptors are generously embedded in the fascia that surrounds tissues and organs, patients often benefit from myofascial release for Ehlers-Danlos syndrome prior to beginning physical therapy. When proprioception is impaired, it can be difficult if not impossible to build stability.
HEDS patients also tend to have reduced tension (stiffness) in the muscle-tendon complex, and tendinopathies are common, contributing to joint instability. Tendinopathies should be addressed before beginning physical therapy. Focused extracorporeal shockwave therapy (ESWT) and eccentric loading protocols can help to restore degenerated tendon tissue, and to treat capsular and ligamentous instability.
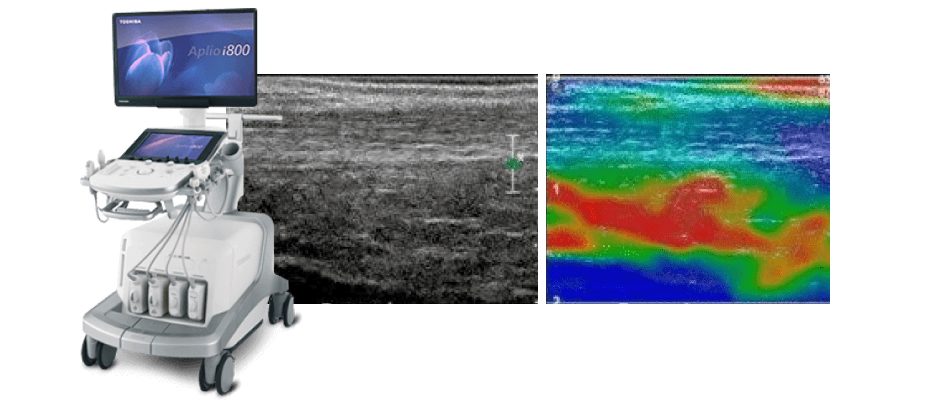
Tissue stiffness and elasticity are mechanical properties that provide passive joint support. A new technology called sonoelastography gives us a valuable diagnostic tool for measuring and evaluating muscle and tendon stiffness. Sonoelastography uses sound waves to assess the elasticity of tissues in response to mechanical pressure.
Ultrasound elastography can measure the thickness and stiffness of deep fascia tissue. Fascia thickness is increased when excess collagen is laid down. Patients with hEDS also have lower tissue stiffness.
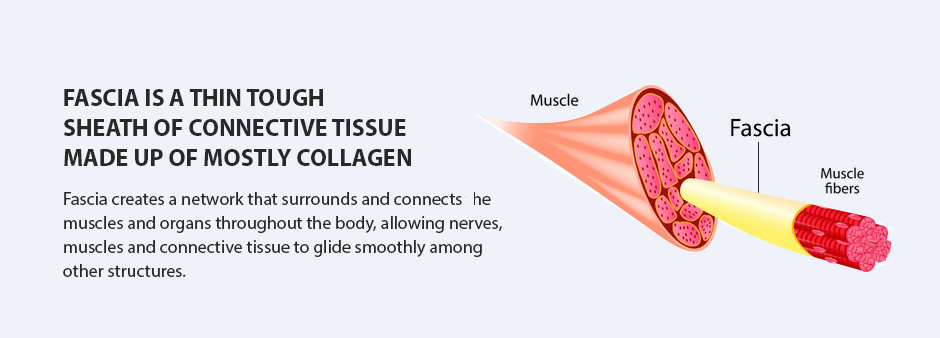
Fascia is a thin tough sheath of connective tissue made up of mostly collagen. Fascia creates a network that surrounds and connects the muscles and organs throughout the body, allowing nerves, muscles and connective tissue to glide smoothly among other structures.
Fascia tissue is made up of multiple collagenous layers, lubricated by a liquid called hyaluronan, derived from hyaluronic acid. Hyaluronan enables fascia to stretch and glide as you move. In addition, fascia is highly innervated with proprioceptors that transmit messages to the brain, making it one of the most significant pain generators in the human body.
One study compared EDS patients with a healthy control group to measure passive resistive torque (PRT) of the plantar flexor muscles – the muscles that act at the ankle to propel you forward and upward. They found evidence that the muscle-tendon unit of hEDS patients appeared to have altered passive properties, thought to be associated with structural modifications in collagen.
Another scientific review points to altered collagen microstructure in hEDS patients, with large, irregularly shaped collagen fibrils that can trigger adhesions within connective tissue.
Research by Dr. Antonio Stecco revealed that smooth fascia gliding is dependent on hyaluronic acid being properly attached to collagen fibers. When deposited abnormally between collagen layers due to structural abnormalities, hyaluronan can clump and cause fascia restrictions that cause pain and impede movement.
Fascia manipulation therapy can help to free up fascia tissue and restore its gliding properties.
While hypermobile EDS directly affects the connective tissue at the joints, it can also impact blood vessels, skin, bones, organs, muscles and nerves. Joint laxity often leads to joint instability, subluxation, and dislocation, and trauma to ligaments, tendons, muscles can occur.
Gastrointestinal issues can arise that cause symptoms like cramping and diarrhea
The cardiovascular system can be affected, causing problems like orthostatic tachycardia and bleeding
Pelvic pain and bladder dysfunction can arise in the genitourinary system
Nervous system disorders may arise, such as fatigue, brain fog, depression and anxiety.
Physical therapy is often the first line of defense for hypermobile joint treatment, aimed at strengthening muscles and connective tissues to promote stability and reduce the risk of joint subluxation.
Prioritize single-joint exercises over compound exercises
Use light weights and higher repetitions
Emphasize good form and control
Avoid joint hyperextension
Include rotator cuff exercises
Include stability exercises for knees and ankles
Use gentle stretching exercises with limited range of motion
Before beginning physical therapy exercises, certain issues may need to be addressed, including hEDS joint pain, load transfer failures, fascia restrictions, tendinopathies and nerve entrapment.
Getting the best care for EDS hypermobility requires a specialist in musculoskeletal disorders who knows how to diagnose and treat the disorder. Run-of-the-mill physical therapists and mainstream medical practitioners rarely have the experience or training to make an accurate diagnosis and provide effective treatment.
Dr. Kalika is a specialist in musculoskeletal disorders like hEDS. He is an expert in diagnostic ultrasonography and sonoelastography, with multiple scientific publications to his credit. Dr. Kalika uses innovative therapies like the Stecco method of myofascial release for Ehlers-Danlos syndrome. He has developed his own unique approach to hypermobility joint syndrome treatment.
Hypermobility joint syndrome treatment at NYDNRehab is geared to reducing hypermobile joint pain and optimizing joint stability, to optimize functional movement and enhance the patient’s quality of life.
Physical therapy clinics are a dime-a-dozen in NYC, but the vast majority of therapists lack the training or access to leverage the most effective treatment technologies. At NYDNRehab, we are continually adding to our treatment toolbox, to offer our patients the best available care.
Prior to initiating repetitive strain injury physical therapy, we use the most advanced high-resolution diagnostic ultrasonography to identify structural damage brought on by your RSI. We then treat your injury with regenerative therapies to put you on the road to healing, followed by repetitive strain injury physical therapy.
If your occupation or activity is causing you pain and limiting your mobility, contact NYDNRehab today, and jump-start the healing process so you can get back to doing the things you love.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































