November 9, 2023

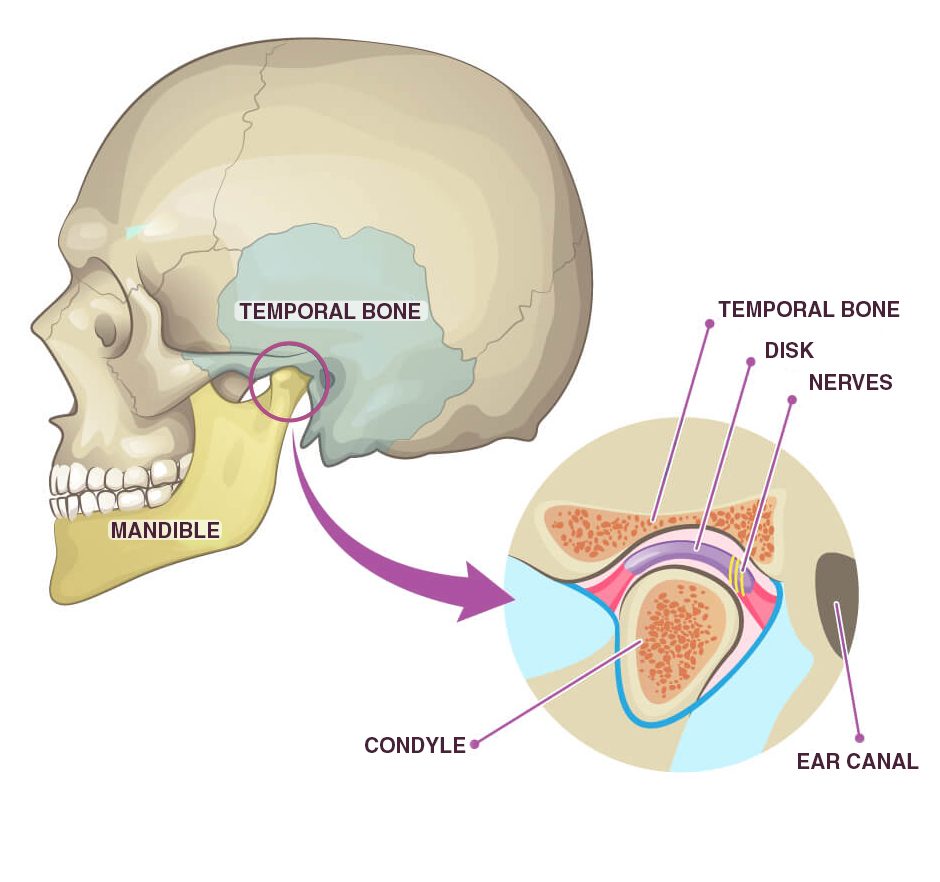
The temporomandibular joint (TMJ) — aka the jaw — is a synovial hinge joint that connects the mandible (jaw bone) to the rest of the skull. The TMJ makes it possible to move your lower jaw in multiple directions and patterns, enabling you to talk, chew, kiss, yawn, and open and close your mouth.
Sometimes the TMJ becomes dysfunctional, causing pain, restricting movement, and making it difficult to speak and chew. When that happens, doctors are often at a loss for solutions, and patients are often referred to a dentist. But dental interventions do not always provide long-term relief.
TMJ physical therapy is frequently the best solution for restoring pain-free functional jaw movement, with outcomes often superior to dental interventions or surgery.
The upper part of the TMJ is formed by the temporal bone, and the lower part is formed by the head of the mandible. The two come together as an articulation between the mandibular fossa, the articular tubercle of the temporal bone, and the condylar process of the mandible. Unlike most synovial joints that are lined with hyaline cartilage, the articular surfaces of the TMJ are lined with fibrocartilage, making it stronger and less elastic than other moveable joints in the body.
TMJ movements are categorized as translational and rotational. Translational jaw movements include protrusion/retraction and lateral deviation. Rotational movements include elevation/depression.
There are over 30 conditions that comprise temporomandibular disorders (TMDs), falling under one of three sub-categories:
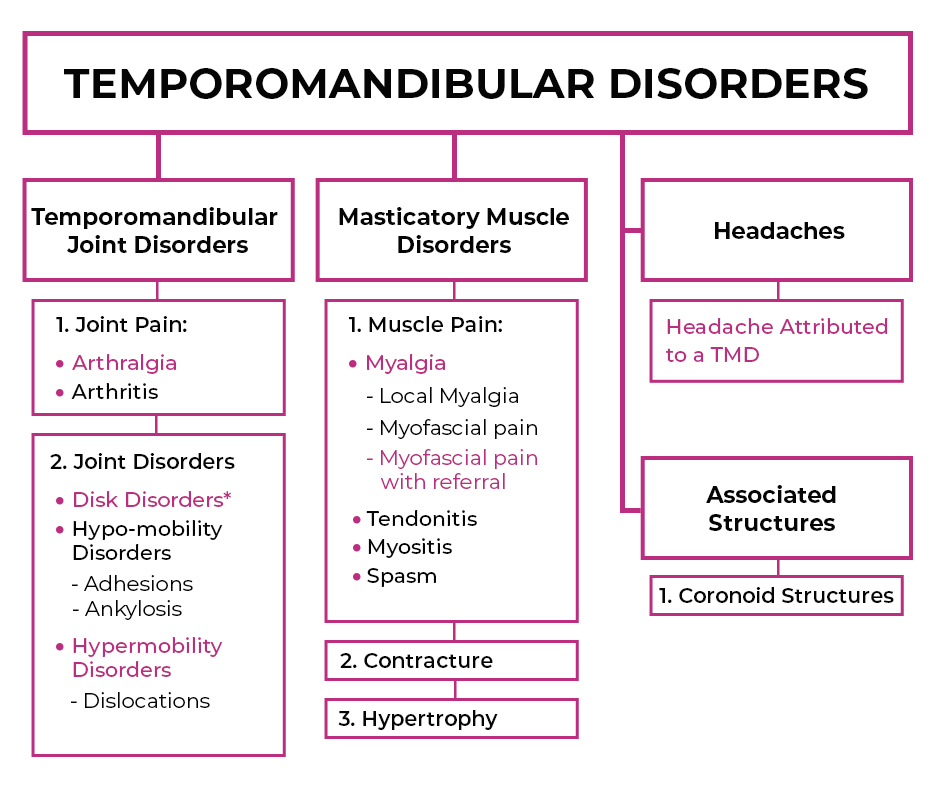
The most common TMD is anterior joint dislocation, an injury that can occur from trauma, yawning, or taking a large bite. In TMJ dislocation, the head of the mandible slides out of the mandibular fossa and shifts forward, making it difficult to close your mouth. In many cases, the exact cause and onset of a TMD is unknown. TMDs are twice as common in women than in men, especially in women aged 35 to 44.
TMD symptoms include:
Some TMDs go away on their own after a few days or weeks, but chronic TMDs may require clinical intervention. Primary care doctors often refer TMD patients to dentists who treat the condition. But while some TMDs are related to tooth alignment and bite, they often have more to do with joint alignment from the feet up, and less to do with dental issues per se.
In some cases, dental work can contribute to TMDs. Procedures like wisdom tooth removal, tooth extraction, poor-fitting crowns and bridges, and orthodontics in teenagers have been linked to the onset of TMDs. Other contributing factors include trauma, stress, and teeth clenching and grinding.

Dental approaches to TMDs include:
When dental interventions fail to resolve TMJ disorders, surgery is often the next step. Oral TMJ surgeries are performed by maxillofacial surgeons. The procedure involves making an incision next to the ear to access the joint. Open TMJ surgery permanently alters the joint, and the procedure cannot be reversed.
There currently exists no long-term research on the safety or efficacy of open TMJ surgery. In fact, evidence suggests that the best surgical outcomes are no better than those achieved through physical therapy. In many cases, surgeries completely fail to resolve TMDs, leaving the patient with irreversible damage that can cause more problems down the road.
Medical interventions for TMDs produce results similar to those for back pain, meniscus tears and hip arthroscopy — interventions are risky, outcomes are negligible, and the changes made can potentially make the problem worse.
One important reason that medical interventions fail is that they set out to treat the symptoms, and not the whole patient. The human body is not like a car, where replacing or repairing a single part fixes the problem. The body is made up of a complex and dynamic network of compound systems, all of them interconnected and interdependent.
Pain and dysfunction often arise in one area of the body due to issues far removed from the locus of pain itself. Without a holistic perspective, doctors may temporarily relieve symptoms, but the underlying cause goes unaddressed.
In the case of TMDs, the position and function of the jaw can be affected by mechanical issues related to other structures, such as:
Few practitioners consider the contribution of mechanical issues to TMJ pain. For example, your brain relies on information sent from mechanoreceptors in your feet to organize your body’s position in space. Poor gait mechanics or foot and ankle injuries can interfere with neural signaling, impacting total body alignment. When your spine is misaligned, it can cause your TMJ to shift out of position.
At the same time, stress and anxiety can cause unnatural contraction of the muscles of your neck and upper back. When coupled with teeth grinding and clenching, along with dental work like orthodontics and wisdom tooth removal, those factors can all contribute to TMJ pain and dysfunction.
Once mechanical deficits and stress are addressed and optimal alignment is restored, your jaw will most likely find its way back to its natural resting position.
Under the holistic care of a knowledgeable and experienced TMJ specialist, TMD sufferers stand a high chance of completely eliminating TMJ pain and dysfunction.
TMDs call for an integrative approach combining multiple evidence-based methodologies:
Extracorporeal shockwave therapy (ESWT) uses high frequency sound waves to stimulate the body’s own reparative mechanisms. It is especially effective for chronic degenerative tendon disorders and myofascial pain syndrome. The procedure is completely safe and non-invasive, and multiple studies (3, 4, 5, 7) have found ESWT to be an effective technology for relieving TMJ muscle pain, especially when used in conjunction with physical therapy.

When subjected to forces from biting, clenching and grinding, the muscles that govern jaw movement can develop myofascial trigger points — tight knots of muscle fibers that cause pain and interfere with muscle function. Trigger points may also arise in the fascia that encases and connects muscles and their surrounding structures. Ultrasound imaging provides a valuable tool for detecting trigger points and guiding dry needling procedures (2). When inserted into the trigger point, thin non-medicated needles evoke a twitch response that relaxes tight fibers and restores muscle function.
INDIBA therapy uses electrical current to restore the ionic charge of damaged cells, to accelerate the healing of injured tissues.
Manual therapy uses mobilization techniques and certain exercises to increase the elasticity of adjacent muscle fibers, to stimulate proprioception and increased production of synovial fluid to ease TMJ pain. One literature review (6) of six separate studies found that manual therapy for TMJ that included massage, TMJ and cervical spine mobilization, myofascial release, trigger point finger pressure, and deep transverse massage, improved mandibular movements and chewing, eased pain, and lowered patient anxiety.
Muscle imbalances are often the root cause of multiple musculoskeletal complaints, and the TMJ is no exception. Cranial manipulation (9) entails both passive and active techniques aimed at restoring balance in the muscles that affect the TMJ.
Prolotherapy injects a biologically neutral solution to irritate slow-to-heal connective tissues, to encourage growth of new normal ligament and tendon fibers. Given the unique fibrocartilaginous makeup of the TMJ, Prolotherapy offers an important adjunct mechanism to promote healing.
TMJ disorders can be debilitating, dramatically interfering with everyday life. While mild forms of TMD sometimes self-resolve, chronic cases can go on for months, with patients enduring painful dental interventions that fail to resolve their condition. Surgery is often proposed as a last resort, with no promise of satisfactory outcomes, and a high risk of irreversible consequences.
At NYDNRehab, we take a holistic approach to treating TMJ. Our clinic is equipped with cutting-edge technologies for treating TMDs without drugs or surgery. Our experienced staff is highly trained and credentialed in advanced therapeutic methods for TMJ rehabilitation. If you are ready to get rid of your TMD for good, contact NYDNRehab today.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































